1. A. plantaris medialis.
2. A. plantaris lateralis.
3. A. peronea (fibularis).
REGIO MALLEOLUS MEDIALIS.
Границы области соответствуют malleolus medialis et tendo Achilii.
В подкожной жировой клетчатке проходит v. saphena magna et n. saphenus. Сanalis malleolaris ограничен malleolus medialis, retinaculum flexorum et tendo Achilii. В канале проходят tendo m. flexor digitorum longus, m. tibialis posterior, m. fleхor halluсis longus, a.v.v. tibialis posterior et n. tibialis. Сосудисто-нервный пучок разделяется на 2 сосудисто-нервных пучка (a.v.v.n. plantares lateralis et medialis).
REGIO PEDIS.
Dorsum pedis.
В подкожной жировой клетчатке располагается rete venosum dorsalis pedis, медиально начинается v. saphena magna, латерально начинается v. saphena parva. Кожа области иннервируется n. saphenus, n. cutaneus dorsalis pedis lateralis (n. suralis), n. peroneus superficialis et profundus.
Основная артерия regio dorsum pedis a. dorsalis pedis.
Ветви a. dorsalis pedis:
1.Aa. tarseae mediales;
2.A. tarsea lateralis;
3.A. arсuata. От нее отходят три aa. metatarseae dorsales разделяющиеся каждая на две aa. digitales dorsales communis, продолжающиеся в aa. digitales dorsales propria;
4. A. metatarsea dorsalis prima;
5. Ramus plantaris pгofundus.
Planta pedis.
Regio planta pedis кровоснабжают aa. plantaгes medialis et lateralis. А. plantaris medialis располагается в sulсus plantaгis media1is. Более кpупная a. plantaris lateralis идет в sulсus plantaris latera1is и участвует в образовании arcus plantaris.
LECTURE 6
OPERATIONS ON VESSELS
Operations on arterial, venous and lymphatic vessels are a large division of modern surgery.
Three basic kinds of operations are carried out on vessels: ligation, vascular suture and vascular plasty.
Bleeding is the basic and most common indication of operations on vessels. The following are classifications of bleeding:
1) On source-arterial,venous,arteriovenous and capillary (parenchymatous);
2) On direction of blood outcome-external and internal;
3) On time of occurrence-initial and secondary.
The arterial bleeding makes up majority of bleedings. According to the Second World War (1941-1945) more than 80% of all bleedings were connected with arterial trunk damages.
Damage of the main arteries includes two dangers for victims:
1) Lethal outcome in connection with bleeding;
2) Necrosis of the distal part of extremity due to failure of collateral arteries blood supply.
The main arteries are divided, the non dangerous for ligation (a.ulnaris, a.radialis, a.tibialis anterior et posterior) and dangerous for ligation (a.subclavia, a.axillaris, a.brachialis, a.femoralis, a.poplitea, a.carotis communis et interna). Angiorrhaphy or vascular plasty are more preferable to make on such arteries. The degree of danger during ligation of the main arteries varies a lot, it depends on the level of ligation and anatomic conditions of collateral blood supply development.
During ligation of dangerous arteries two ligatures impose and there is a cross vessel between them for desimpatisation of nerve adventicia, expansions of collaterals and collateral blood supply.
V.A. Oppel ligates the same vein for blood balance regulation.
It is necessary to apply a vessel suture for stopping bleeding from dangerous vessels. If the vascular suture cannot be made at once, it is possible to make a temporary repair with the help of a tube made from synthetic material (polychlorvinil, silicon) for 72 hours. Washed with a solution of heparinum the tube is inserted in distal and proximal ends of the vessel and is fixed by ligatures.
The approach on a blood vessel is usually carried out by level-by-level section of tissues on the projective lines.
Ligation of vessels is made on a wound and at a distance, from a distance to the place of vessel damage.
Indications of ligation of arteries on extension:
1) Impossibility of vessel ligation on a wound when the vessel lays in thickness of an inflammatory infiltrate;
2) Traumatic aneurysms;
3) Amputation of extremity at gangrene, anaerobic infection.
METHODS OF FINAL HEMOSTASIS
Ligating of vessels in a wound is the most reliable way of controlling bleeding. The central and peripheral ends of a bleeding vessel are picked up, grasped with haemostatic clamps and ligated.
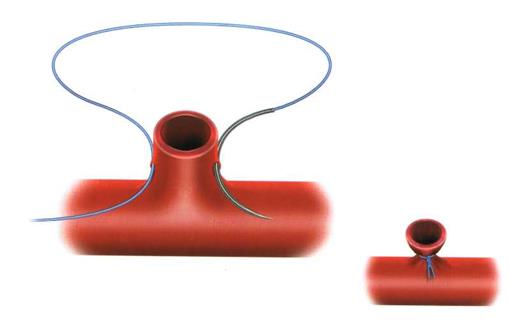

Fig. 14.Vascular ligations.
The central end is ligated twice during ligation of large arterial vessels. The central end is ligated by placing a suture for the second time in order to avoid slipping of ligatures and bleeding. Damaged vessels of small caliber can be grasped by haemostatic clamps and made vasoversion by rotary movements.
Sometimes if small wounds and damaged vessels of small caliber are present, it is possible to make tamponade of a wound. Frontal and back tamponade of a nose during nasal bleeding is a typical example of bleeding control.
VASCULAR SUTURE
The basic indication of angiorrhaphy is restoration of the main arteries’ permeability. There are manual vascular and mechanical vascular sutures.
The manual vascular suture may be lateral and circular. The mechanical vascular suture is placed by means of angiorrhaphy apparatus.
The demands of an angiorrhaphy are as follows:
1. Hermetism. It is reached by removal of vessel adventicia of 2-3 mm from the end, dense contact of intima, applying of close (through 1 mm) continuous blanked suture.
2. Prophylaxis of a thrombogenesis. It is reached by application of anticoagulants. The vascular suture should not break blood current (absence of narrowing and turbulence); suture material should be as small as possible in a lumen of vessel.
3. Prophylaxis of vessel lumen narrowing. It is reached by applying sutures which are stretched on the wall of the vessel, and the continuous vascular suture does not allow the wall of the vessel to constrict back to its former size.
Vascular sutures are placed manually with the help of atraumatic needles. A mechanical vascular suture is perfect and does not narrow vessel’s lumen but its used only during planned operations and the vessel's diameter must be more than 2,5 mm.
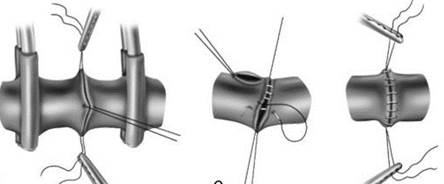
Fig. 15. Vascular sutures.
VASCULAR SUTURE BY CARREL
1. Approach to a vessel. A projective line is used for approaching a vessel. Approach includes level-by-level section of tissues on a line or at a distance of 1-2 cm from it: skin, hypodermic fatty tissue, superficial fascia, own fascia (forming fascial cover).
2. Mobilization. It is rising of a vessel and its accompanying vessels and nerves from a fascial bedsore. This stage also includes applying of Hepfner’s artery forceps at a distance of 1-2 cm from the ends of a vessel.
3. Angiorrhaphy. Excision of a vessel's damaged ends and removal of 2-3mm adventitia. The ends of the vessel are fixed by applying 3 sutures by Carrel. The vessel is sutured between fixating sutures by a continuous blanket suture of 1 mm using one of the strings from guy suture.
4. Level-by-level suturing of a wound.
VASCULAR PLASTY
When there is a big defect present transplantats from biological material is carried out. Autoveins are usually used (v.saphena magna, v.basilica).
Auto- and allotransplants of arteries and veins are used as transplants in vessel surgery; isotransplants made from synthetic materials are used. Reconstruction is made by applying an anastomosis of end-to-end or transplants suturing.
STENTING OPERATIONS
Heart surgery using stents is an indispensable and lifesaving surgical procedure mostly used when the patient has severe heart blockage, risk of a heart attack or arterial blockage.
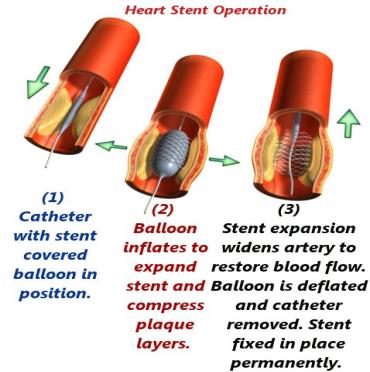
Fig. 16. Heart Stent Operation
ЗАНЯТИЕ № 6.
ОПЕРАЦИИ НА СОСУДАХ.
Операции на артериальных, венозных и лимфатических сосудах составляют крупный раздел современной хирургии.
На сосудах выполняют 3 основных вида операций: перевязку, сосудистый шов и сосудистую пластику.
Основным и наиболее частым показанием к операциям на сосудах является кровотечение.
Различают следующие виды кровотечений:
1) по источнику – артериальное, венозное, артериально-венозное и капиллярное (паренхиматозное);
2) по направлению вытекания крови – наружное и внутреннее;
3) по времени возникновения – первичное и вторичное.
Артериальное кровотечение составляет подавляющее большинство кровотечений. По данным ВОВ (1941-1945 г.г.) более 80% всех кровотечений было связано с повреждением артериальных стволов.
Повреждение магистральных артерий представляет две опасности для пострадавших.
1) угрозу смертельного исхода в связи с кровотечением;
2) возможность омертвения дистальной части конечности за счет недостаточности ее питания коллатеральными артериями.
Магистральные артерии разделяются на «безопасные» для перевязки (a.ulnaris, a.radialis, a.tibialis anterior et posterior) – и «опасные» для перевязки (a.subclavia, a.axillaris, a.brachialis, a.femoralis, a.poplitea, a.carotis communis et interna). На данных артериях предпочтительнее производить наложение сосудистого шва или сосудистую пластику. Степень развития гангрены в случаях перевязки магистральных артерий варьирует в очень широких пределах, в зависимости от уровня перевязки артерий и анатомических условий для развития коллатерального кровоснабжения.
При перевязке «опасных» артерий накладывают две лигатуры и между ними пересекают сосуд для десимпатизации нервов адвентиции, расширения коллатералей и улучшения коллатерального кровоснабжения.
Для выравнивания кровяного баланса В.А. Оппель предложил одновременно перевязывать одноименную вену.
Для остановки кровотечения из опасного для перевязки сосуда, хирург должен стремиться к восстановлению непрерывности поврежденного сосуда с помощью сосудистого шва. Если сосудистый шов нельзя выполнить сразу, на относительно короткий промежуток времени можно произвести метод временного протезирования до 72 часов с помощью трубки из синтетических материалов (полихлорвинил, силикон). Промытую (раствором гепарина) трубку вводят в дистальный и проксимальные концы и закрепляют ее лигатурами.
Подход к кровеносному сосуду обычно осуществляется послойным разрезом тканей по проекционным линиям, соответствующим его проекции на кожу.
Если разрез производят строго по проекционной линии, такой доступ называется прямым. Если разрез для обнажения магистрального сосуда производится несколько в стороне от проекционной линии, то такой разрез называют окольным. Например, при обнажении плечевой артерии в средней трети нужно помнить о срединном нерве, находящемся спереди от артерии. Окольный доступ к плечевой артерии осуществляется через влагалище двуглавой мышцы плеча, предотвращающей в последующем вовлечение срединного нерва в послеоперационный рубец.
Показаниями к обнажению и перевязке артерии на протяжении служат:
1) невозможность перевязки сосуда в ране при сильном размозжении тканей, когда эрозированный сосуд находится в толще воспалительного инфильтрата;
2) травматические аневризмы;
3) ампутация конечности при самопроизвольной гангрене, анаэробной инфекции, когда наложение жгута противопоказано.
Перевязка на протяжении по сравнению с перевязкой сосуда в ране применяется значительно реже из-за возможности развития гангрены в ближайшем периоде после операции; возникновения в отдаленные сроки при сохранении жизнеспособности конечности, так называемой «болезни перевязанного сосуда», которая проявляется быстрой утомляемостью конечности, периодически возникающими болями, атрофией мышц из-за относительной недостаточности кровоснабжения тканей.
Перевязку сосудов производят в ране и на протяжении, то есть на некотором расстоянии от места повреждения сосуда.
Дата: 2019-03-05, просмотров: 475.