LECTURE 1
SEPERATION OF THE TISSUES AND THE TECHNIQUES OF APPLYING SUTURES ON THE TISSUES.
MAIN PRINCIPLES OF CLOSING OF THE WOUND
The edges of the wound must never be stretched while stitching. Rather sharp retractors may be used instead of forcible stretching. Foriegn bodies like even the ligature materials must nevr be left in the wound for a very long time as it may hinder the the normal wound repair. Because of the same reason, continuous sutures must be used while suturing the subcutaneous fatty tissues. So, the suture ends are deduced on the skin so that they can be taken out easily if necessary.
· INTERRUPTED SUTURES:
The interrupted sutures consist of seperate stitches. Placing of each of the stitch includes 4 moments: insert needle, prick out, passing and stretching of the suture material and then to tie a knot. Inserted sutures are more reliable because even if one of the sutures is cut-off, the other knots continue to hold the wound edges. Similar sutures can be applied on infected wounds, as the probability of diffusion of the microorganisms along the line of interrupted sutures is very less. Interrupted sutures are usually used on the skin and the aponeurosis and are practically not applied in the practice of cosmetic surgery.
· SIMPLE INTERRUPTED SUTURE:
It provides the exact connection of the wound edge with the surrounding healthy tissues and edges of the epithelial layer.
Technique: The wound edges are turned back. The needle is inserted into the epithelial layer, 0,5-1 cm, away from the edge of the wound. While holding the skin with the forceps, the needle is passed through the length of the layers of the skin (The direction of the hand movement has to correspond to the curvature of the needle). Then the needle is passed through the subcutaneous tissues, turned towards the wound and tightly held in such a way that the edges are closer. Then the needle is taken out the same way as while it was inserted in. The stitches must strictly correspond with the symmetrical parts of both the sides of the wound. In this way, same amount of tissues develop along the suture. The needle mist is passed in two stages: insertion and extraction with the help of independent hand movements.
· CONTINUOUS SUTURES:
Technique: The first step of application of the continuous sutures is the same as that of in the application of interrupted sutures, and then the same suture material is used to stitch the whole length of the wound. Therefore, it is important to pass the needle through symmetrical depth and breadth. Usually the needle is inserted 1cm away from the edge of the wound and is retracted the same way, 1cm away from the edge of the wound. After each stitch, the assistant intercepts the thread and ties a knot. The sutures are applied 1-2 cms away from each other. During the last stitch, the thread is not intercepted but tied up with the help of double surgical knots.
Continuous mattress sutures are usually used to stitch vessels, peritoneum, stomach wounds and intestines, since the application of these sutures are much simpler and lesser time- consuming than the knot.
EACH OF THE ABOVE MENTIONED SUTURES IS ALWAYS FINISHED BY TYING A KNOT!
KINDS OF KNOTS
There are 3 types of knots:
· Surgical knot
· Simple knot
· Marine knot
The surgical knot is characterised by the edouble crossing of the thread and is always finishe with a simple crossing. The surgical knot is very strong and so it is uasually used to ligate large vessels.
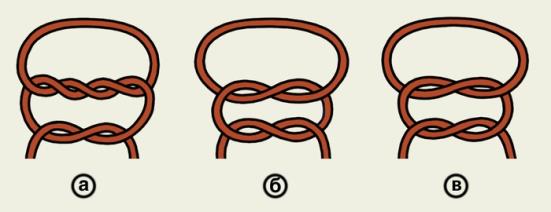
Fig. 4. Kinds of knots,
a) surgical (friction) knot (хирургический узел)
b) simple knot (простой узел)
c) Marine knot (морской узел)
ЗАНЯТИЕ № 1.
РАЗЪЕДИНЕНИЕ ТКАНЕЙ.
Разъединение мягких тканей при операциях производится с помощью режущих инструментов – скальпеля и ножниц. Общий принцип разъединения тканей заключается в строго послойном разрезе. Направление разрезов должно соответствовать ходу крупных сосудов и нервов во избежание их повреждения, а также с учетом расположения так называемых линий Лангера, характеризующих направление соединительно-тканных волокон глубокого слоя кожи.
Рассечение мягких тканей.
Фасции. После разреза кожи с подкожной жировой клетчаткой оперирующий (вместе с ассистентом) в центре приподнимает фасцию двумя хирургическими пинцетами, надсекает её и вводит в разрез фасции желобоватый зонд. Проводя скальпель лезвием кверху по желобку зонда, фасцию рассекают на всём протяжении разреза кожи.
Мышцы. С целью предупреждения образования послеоперационных грыж при операциях на органах брюшной полости мышцы передней брюшной стенки стараются не пересекать, их тупо раздвигают по направлению волокон.
Брюшина. Париетальный листок брюшины, надсечённый между двумя анатомическими пинцетами, разрезают ножницами на протяжении всей длины кожной раны, подняв его на введённых в полость брюшины II и III пальцах левой руки хирурга.
Кровеносные сосуды. Перерезаемые поверхностные сосуды ассистент придавливает марлевыми шариками. После этого кровотечение тут же останавливают наложением кровоостанавливающих пинцетов Пеана или Кохера с последующей перевязкой сосудов. В некоторых клиниках предпочитают осуществлять гемостаз с помощью диатермокоагуляции.
СОЕДИНЕНИЕ ТКАНЕЙ.
Соединение тканей может производиться ручным наложением швов, созданием механического шва с использованием различных сшивающих аппаратов либо склеиванием (полимеризация жидких мономеров после контакта с тканевыми жидкостями, сопровождающаяся быстрым затвердеванием). Выбор того или иного метода зависит от вида тканей, сложности операции и оснащённости клиники. При наложении ручного шва применяются преимущественно узловые и непрерывные швы.
Ручное наложение швов — самый частый способ соединения тканей. Швы накладывают с помощью иглы, иглодержателя и шовного материала.
Выбор шовного материала (шёлк, кетгут, проволока и др.) зависит от требований, предъявляемых к шву, и от качеств, достоинств и недостатков каждого из этих материалов. В то время как шёлковая нить в тканях организма почти не рассасывается, кетгут обладает способностью рассасываться в течение 12—24 дней (в зависимости от толщины нити и способа её предварительной обработки), однако прочность шва и надёжность узла при использовании кетгута ниже. В связи с этим там, где нужна особая прочность при соединении тканей (например, швы на апоневроз при грыжах), пользуются чаще шёлком; если выгодно наложить швы из быстро рассасывающегося материала и избежать присутствия инородного тела в тканях (швы на стенку почечной лоханки, мочевого пузыря), применяют кетгут.
Режущие, трёхгранные в сечении, хирургические иглы применяют для прошивания относительно плотных тканей (кожа, апоневроз). Круглые в сечении, колющие иглы употребляют при наложении шва на относительно податливые ткани (кишки, мышцы).
Иглу зажимают концом иглодержателя на границе средней и задней (ближайшей к ушку) её трети. Нить длиной 15-18 см (для узловых швов) или значительно большей длины (для непрерывных швов) вдевают в ушко хирургических игл сверху. Для кишечных швов иногда применяют и прямые иглы, которыми шьют без иглодержателя.
Простой узловой шов.
Простой узловой шов должен обеспечивать соединение краёв раны с точным сближением соотносящихся тканевых элементов и краёв эпителиального слоя.
Техника. Отвернув край раны, делают вкол в эпителиальный слой у её края, отступив от него на 0,5—1 см, насаживая пинцетом кожу на иглу и одновременно проводя иглу (движением руки, соответствующим кривизне иглы) через всю толщу кожи. Затем иглу косо проводят в подкожной ткани, поворачивают к ране и проводят вплотную с дном раны. Выкол делают из глубины кнаружи тем же приёмом. Игла должна проходить строго симметрично и в тканях другого края раны. В шов при этом попадёт одинаковое количество тканей. Игла через ткани должна проводиться в два этапа (вкалывание и выведение) самостоятельными движениями.
НЕПРЕРЫВНЫЙ ШОВ.
Техника. Первый стежок непрерывного шва завязывают так же, как узловой, затем прошивают той же ниткой всю длину раны, при этом все слои раны нужно захватывать равномерно по глубине и ширине. Обычно иглу вкалывают в кожу на расстоянии 1 см от края разреза и на таком же расстоянии выкалывают. После каждого стежка ассистент двумя пинцетами перехватывает нитку и тем самым стягивает рану. Швы накладывают на расстоянии 1—2 см друг от друга. При последнем стежке нити не перехватывают и заканчивают шов двойным хирургическим узлом.
Непрерывный матрацный шов применяют при сшивании сосудов, брюшины, ран желудка и кишечника, так как на наложение такого шва затрачивается меньше времени, чем на узловой.
Любой вид шва заканчивается завязыванием узла.
Виды узлов.
Различают несколько видов узлов: простой, обвивной, женский, морской, хирургический.
Хирургический узел характеризуется двукратным перекрещиванием нити и всегда заканчивается обыкновенным перекрещиванием. Этим он отличается от других видов узлов. Хирургический узел очень прочен и особенно показан при перевязке крупных сосудов.
Снятие кожного шва.
Кожный шов снимают следующим образом: приподняв хирургическим пинцетом узел, несколько вытягивают лигатуру из канала шва, с тем, чтобы при извлечении не протаскивать через этот канал часть нити, находившуюся вне кожи. Затем срезают нить ниже узла и вытягивают шов целиком.
В клинических условиях швы удаляют на 3—10-й день после операции, т.е. когда прочность рубца достигает 5—10% нормальной прочности тканей. Удерживание краёв раны в течение длительного времени без ухудшения состояния рубца возможно только внутрикожным косметическим швом.
Следует отметить целесообразность раннего удаления швов (шовный материал, находящийся в ране, нарушает процесс формирования соединительной ткани), что уменьшает частоту нагноений, ускоряет заживление и приводит к формированию нежного послеоперационного рубца. После удаления швов устраняется сдавление тканей, улучшается лимфо- и кровообращение. Шовные метки (следы, возникающие в результате давления швов на кожу) более выражены при натяжении раны, отёке, инфицировании, при вовлечении больших тканевых поверхностей.
LECTURE 2
DELTOID REGION
The deltoid region indicates the localisation of the deltoid muscles and the humeral articulation. The proper fascia of the deltoid region forms the vagina for the m. Deltoideus. The processes penetrating through the muscles and divide it into fascicles extends from the fascia to the muscles. Between m.deltoideus and the humeral bone is located the cellulose space spatium subdeltoideum, through which passes n.axillaris and a.Circumflexa humeri posterior.
HUMERAL ARTICULATION
Caput humeri and cavitas glenoidealis scapulae form the humeral articulation.
The articulation is held in place with the help of 5 ligaments: lig. Coracoacromiale, lig. Coracohumerale, lig. Glenohumerale superioris, lig. Glenohumerale inferioris, lig. Glenohumerale media.
The synovial bursa is located near the joint. Two of these bursas do not communicate with the joint cavity: bursa subdeltoidea, bursa subacromialis. Bursa subscapularis and bursa subcoracoidea communicate with the joint cavity. The joint capsule is attached to the surgical neck of the humeral bone. The cavity of the humeral joint is expanded with the help of three rotations: recessus axillaris, recessus subscapularis, and recessus intertubercularis.
SUBCLAVIAN REGION
The layer-by-layer structure of this region is represented by the skin, subcutaneous fatty tissue, superficial fascia, proper fascia, m.pectoralis major et minor.
There are three triangles in the subclavian region:
1. Trigonum claviculopectorale [bordered superiorly by the clavicle, medially by the sternum, laterally downwards by m.pectoralis minor]
2. Trigonum pectorale [corresponds to the borders of m.pectoralis minor]
3. Trigonum subpectorale [corresponds to the borders of fossa axillaris]
The important neurovascular fascicle in the subclavian region is a.v. subclavia, plexus brachialis. The continuity of a. Subclavia is a. Axiallaris, which in turn continues as a. Brachialis.
The proximal borders of the trunk of a.axillary is the lateral border of the first rib, and the distal border is the inferior border of m. Teres major (place of beginning of a. Brachialis)
A. axillaris is located in the axillary cavity medial to the humeral joint cavity and the humeral bone; medially and anteriorly to the artery are located v. Axillaris and from all the three sides is surrounded by the trunk of plexus brachialis; inferiorly the neuro vascular fascicle is covered by skin, fascia and mass of fatty tissues, which consist of the lymph nodes.
A. axillaris gets divided into three sections:
1) From the clavicle, medial border of the sternum upto the superior border of m. Pectoralis minor (trigonum claviculopectorale)
2) Behind m. Pectoralis minor (trigonum pectorale)
3) From the inferior border of m. Pectoralis minor upto the inferior border of m. Pectoralis major (trigonum subpectorale)
The branches of a. Axillaris in the claviculopectoral triangle are:
1. A.thoracic superior gets divided in m. Subclavius, m. Pectoralis major et minor, m. Serratus anterior superior, m. Intercostalis
2. A. Thoracoacromialis takes part in the nourishment of the humeral articulation, m. Deltoideus, m.pectoralis major and minor.
The branches of a. Axillarisin the pectoral triangle are:
3. A. Thoracica lateralis descends down along the lateral wall of the thorax and gives branches to the mammary glands and the surrounding muscles.
The branches of a. Axillaris in the subpectoral triangle or in the axillary fossa are:
4. A. Subscapularis, which is the largest branch of a. Axillary, starts from the inferior border m. Subscapularis, descends along this muscle and divides into two trunks:
a) A. Circumflexa scapulae passes through the trilateral foramen onto the dorsal surface of the scapula
b) A. Thoracodorsalis passes along the posterior surface of the thorax
5. A. Circumflexa humeri posterior passes posteriorly, into the quadrilateral foramen, curves around the surgical neck of the humeral bone and is supplies m. Deltoideus.
6. A. Circumflexa humeri anterior passes in the lateral direction, circumflexes around the the surgical neck of the humeral bone anteriorly, and anastomizes with a. Circumflexa humeri posterior.
AXILLARY FOSSA
The axillary fossa is cone shaped. It is bordered: anteriorl by the inferior border of m. Pectoralis major, posteriorly by m. Latissimus dorsi, medially by the line that joins the borders of these muscles on the thorax, laterally by the line that joins borders of these muscles on the humeral bone.
The walls of the axillary fossa are: anterior- m.pectoralis major et minor; posterior- m.latissimus dorsi, m. Teres major et minor, m.subscapularis; lateral- m. Corachobrachialis; medial- m. Serratus anterior superior.
On the posterior wall of the axiallary fossa are located two foramens: trialteral and quadrialateral. The trilateral foramen is bordered: superiorly by m. Teres minor, m. Subscapularis; inferiorly by m. latissimus dorsi, m. Teres major; laterally bycaput longum m. Triceps brachii. A. Circumflexa scapula passes through this foramen.
The quadrialteral foramen is bordered: superiorly by m. Teres minor, m. Subscapularis; inferiorly m.latissimus dorsi, m. Teres major; laterally by the humeral bone; medially by the caput longum m. Triceps brachii. N. axillaris and a. circumflexa humeri posterior pass through this foramen.
The important neuro-vascular fascicle in this fossa consist of the superficially located v. Axillaris, laterally and deeply located a. Axillaris, which is surrounded by three fascicles of the brachial plexus (lateral, medial and posterior). From the fascicle of the brachial plexus begins the nerves in the axillary fossa. From the posterior bundle starts n. radialis, n. axillaris; from the medial bundle starts medial radix of n. medianus, n. ulnaris, n. cutaneus brachii medialis, n. cutaneus antebrachii medialis; from the lateral bundle starts the lateral radix of n. medianus, n. musculocutaneus.
In the subcutaneous fatty layer are located 5 groups of lymph nodes: nodi. Lymphatici axillaris lateralis, nodi lymphatici axillaris medialis (pectoralis), nodi lymphatici axillaris centralis, nodi lymphatici axillaris subscapularis, nosi lymphatici axillaris apicalis
BRACHIAL REGION
This region is limited: superiorly by the line, that joins the borders of m. Pectoralis major and m. Latissimus dorsi; inferiorly by the line that passes at a level of two fingers above the humeral epicondilus. The skin, subcutaneous fatty tissues, superfiscial and proper fascia represent the layers of this region. The proper fascia surrounds the muscles and the neuro-vascular bundles of the arm.
Through the subcutaneous fatty tissues pass the superfiscial veins laterally, v. Cephalica passes through the lateral bicipital sulcus; and medial to the medial bicipital sulcus passes v. Basilica together with n. cutaneous antebrachii medialis. The skin on the arm is innervated b n. cutaneous brachii lateralis, medialis et posterior.
The important neuro-vascular bundles in the arm are a.v.v. brachiales and n. medianus. The bundle passes through the medial bicipital sulcus. In the upper third of the arm, the nerve is located lateral to the artery, and in the middle third on the artery, and in the lower third medially from the artery. The second neuro-vascular bundle in this region are the a.v.v collateralis ulnaris superior and n. ulnaris, which in the middle third passes through the bed formed by m. Triceps brachii. The third neuro-vascular bundle in the region consists of a.v.v profunda brachii and n. radialis that are located in the posterior surface of the arm and passes through the humero-muscular canal (spiral canal, canal of n. radialis). M. Triceps brachii and the humerus bone form the canal. The branches of a. Brachialis- a. Collateralis ulnaris superior and inferior, and a. Profunda brachii and its branches a. Collateralis media and a. Collateralis radialis accomplish the collateral blood supply to the arm.
Fig. 6. Fossa axillaris.
Fig. 7. Regio brachii.
ЗАНЯТИЕ № 2.
REGIO DELTOIDEA.
Regio deltoidea соответствует месту расположения m.deltoideus et articulatio humeri. Собственная фасция regio deltoidea образует влагалище для m.deltoideus. От фасции к мышце отходят отростки, проникающие в мышцу и разделяющие ее на пучки. Между m.deltoideus и os humeri находится клетчаточное пространство spatium subdeltoideum, в котором проходят n. axillaris et a. circumflexa humeri posterior.
ARTICULATIO HUMERI.
Articulatio humeri образован caput humeri et cavitas glenoidalis scapulae.
Articulatio humeri укреплен пятью связками: ligamentum coracoacromiale, ligamentum coracohumerale, ligamentum glenohumerale superius, ligamentum glenohumerale inferius, ligamentum glenohumerale medium.
Вблизи сустава располагаются синовиальные сумки. Две из них не сообщаются с полостью сустава: bursa subdeltoidea, bursa subacromialis. Bursa subscapularis et bursa subcoracoidea с полостью сустава сообщаются. Суставная капсула прикрепляется к анатомической шейке os humeri. Полость аrticulatio humeri расширена за счет трех заворотов: recessus axillaries, recessus subscapularis, recessus intertubercularis.
REGIO SUBCLAVIA .
Послойное строение области представлено кожей, подкожной жировой клетчаткой, поверхностной фасцией, собственной фасцией, окружающей m. pectoralis major et minor.
В regio subclavia выделяют три треугольника:
1. Trigonum clavipectorale – ограничен сверху - clavicula, медиально – sternum, латерально снизу - m. pectoralis minor.
2. Trigonum pectorale – соответствует границам m. pectoralis minor.
3. Trigonum subpectorale – соответствует границам fossa axillaries.
В данной области основным сосудисто-нервным пучком является a.v. subclavia et plexus brachialis. Непосредственным продолжением a. subclavia является а. axillaris, которая продолжается в a. brachialis.
Проксимальной границей ствола подмышечной артерии служит наружный край I ребра, дистальной границей - нижний край m. teres major (место начала a. brachialis).
A. axillaris расположена в cavitas axillaris медиально от плечевого сустава articulation humeri и os humeri; спереди и медиальнее ее располагаются v. axillaris и с трех сторон - нервные стволы plexus brachialis; снизу этот сосудисто-нервный пучок прикрыт кожей, фасцией и скоплением жировой клетчатки, содержащей лимфатические узлы.
По ходу а. axillaris различают три отдела:
I) от ключицы, медиального края грудины до верхнего края m. pectoralis minor (trigonum clavipectorale);
2) позади m. pectoralis minor (trigonum pectorale);
3) от нижнего края m. pectoralis minor до нижнего края m. pectoralis major (trigonum subpectorale).
Ветви а. axillaris в trigonum clavipectorale:
1. А. thoracica superior разветвляется в m. subclavius, m. pectoralis major et minor, m. serratus anterior superior, m. intercostalis.
2. А. thoracoacromialis, принимает участие в питании articulatio humeri, m. deltoideus, m. pectoralis major et minor.
В trigonum pectorale:
3. А. thoracica lateralis, спускается по боковой стенке грудной клетки и посылает ветви к glandula mammae и окружающим мышцам.
В trigonum subpectorale (fossa axillaries):
4. А. subscapularis, самая крупная ветвь a. axillaris, начинается у нижнего края m. subscapularis, спускается вдоль этой мышцы и делится на два ствола:
а) a. circumflexa scapulae уходит через foramen trilaterum на дорсальную поверхность лопатки;
б) a. thoracodorsalis переходит на заднюю поверхность грудной клетки.
5. А. circumflexa humeri posterior, идет назад в foramen quadrilaterum, обходит сзади хирургическую шейку os humeri и кровоснабжает m. deltoideus.
6. А. circumflexa humeri anterior, идет в латеральном направлении, огибает хирургическую шейку os humeri спереди, анастомозируя a. circumflexa humeri posterior.
FOSSA AXILLARIS .
Fossa axillaries имеет форму конуса. Она ограничена: спереди нижний край m. pectoralis major, сзади m. latissimus dorsi, медиально линия соединяющая края этих мышц на грудной клетке, латерально – линия соединяющая края этих мышц на os humeri.
Стенки fossa axillaries: передняя – m. pectoralis major et minor; задняя – m. latissimus dorsi, m. teres major et minor, m. subscapullaris; латеральная – m. coracobrachialis; медиальная - m. serratus anterior superior.
На задней стенке fossa axillaries выделяют два отверстия foramen trilaterum et quadrilaterum. Foramen trilaterum ограничено сверху - m. teres minor, m. subscapullaris; снизу - m. latissimus dorsi, m. teres major; латерально – caput longum m. triceps brachii. Через него проходит a. circumflexa scapula.
Foramen quadrilaterum ограничено сверху - m. teres minor, m. subscapullaris; снизу - m. latissimus dorsi, m. teres major; латерально – os humeri; медиально - caput longum m. triceps brachii. Через него проходит n. axillaris et a. circumflexa humeri posterior.
Основной сосудисто-нервный пучок ямки состоит из поверхностно расположенной v. axillaris, латерально и глубже расположена a. axillaris, которая окружена тремя пучками plexus brachialis (латеральным, медиальным, задним). Из пучков plexus brachialis в fossa axillaris начинаются нервы. Из заднего – n. radialis, n. axillaris; из медиального – radix medialis n. medianus, n. ulnaris, n. cutaneus brachii medialis et n. cutaneus antebrachii medialis; из латерального – из radix lateralis n. medianus, n. musculocutaneus.
В жировой клетчатке fossa axillaris располагаются 5 групп лимфатических узлов: nodi lymphatici axillaris lateralis, nodi lymphatici axillaris medialis (pectoralis), nodi lymphatici axillaris centralis, nodi lymphatici axillaris subscapularis, nodi lymphatici axillaris apicalis.
REGIO BRACHII .
Область ограничена: вверху линией соединяющей края m. pectoralis major et m. latissimus dorsi; внизу – линией, проходящей на 2 поперечных пальца выше epicondilus os humeri. Слои области представлены кожей, подкожной жировой клетчаткой, поверхностной и собственной фасциями. Собственная фасция (fascia brachii) окружает мышцы и сосудисто-нервные пучки плеча.
В подкожной жировой клетчатке проходят поверхностные вены – латерально, по sulcus bicipitalis lateralis проходит v. сephalica; и медиально по sulcus bicipitalis medialis проходит v. basilica вместе с n. Сutaneus antebrachii medialis. Кожа плеча иннервируется n. cutaneus brachii lateralis, medialis et posterior.
Основным сосудисто-нервным пучком плеча является a.v.v. brachiales et n. medianus. Он проходит по sulcus bicipitalis medialis. В верхней трети плеча нерв располагается латерально от артерии, в средней трети на артерии, а в нижней трети плеча медиально от артерии. Вторым сосудисто-нервным пучком является n. ulnaris et a.v.v. collaterals ulnaris superior, которые в средней трети плеча переходят в ложе m. triceps brachii. Третий сосудисто-нервный пучок, состоящий из a.v.v. profunda brachii et n. radialis располагается на задней поверхности плеча в canalis humeromuscularis (canalis spiralis, canalis n. radialis). Канал образован m. triceps brachii et os humeri. Коллатеральное кровоснабжение плеча осуществляется ветвями a. brachialis – a. collateralis ulnaris superior et inferior, а также a. profunda brachii и отходящими от нее a. collateralis media et a. collateralis radialis.
LECTURE 3
FOSSA CUBITI
The cubital fossa is limited above by m. Brachioradialis laterally, by m. Biceps brachii medially, and below by m. Brachioradialis laterally, by m. Pronator teres medially. The layers of this region are: skin, subcutaneous fatty layer, the proper fascia, the surrounding neuro-vascular bundles and the muscles of the region.
In the subcutaneous fatty layer is located the superficial veins and the cutaneous nerves: laterally - v. Cephalica, n. cutaneous antebrachii lateralis (enters into the cubitalfossa in between m. Biceps brachii and m. Brachialis); medially - v. Basilica and n. cutaneouss antebrachii medialis. The veins form two different anastomoses between themselves:
1. < N > shaped (v. Mediana cubiti)
2. < M > shaped (v. Mediana cephalica, v. Mediana basilica, v. mediana antebrachii)
Through the cubital fossa passes two neuro-vascular bundles. Laterally - n. radialis and a.v. collateralis radialis. The nerve leaves the fossa in between m. Brachialis and m. Brachioradialis. It branches into superficial ramus of n. radialis, which goes along the anterior surface of the forearm and the deep ramus of n. radialis, which passes through the supinator canal on the posterior surface of the forearm. The medial neuro-vascular bundle is formed by a.v.v brachialis and n.nmedianus. The artery passes medially from m. Biceps brachii, and the nerve passes 0,5-1,0 cm medially from the artery.
On the posterior surface of the cubital region is located the osteofibrous canal, which is formed by the medial epicondle of the humerus and the olecranon of the ulna. Through the canal passes n. ulnaris and a.v. collateralis ulnaris superior.
CUBITAL ARTICULATION
The cubital articulation is formed by 3 bones: The humerus, the ulna and the radius.
The joint is strengthened by 3 ligaments: lig. Anulare radii, lig. Collaterale ulnare, lig. Collaterale radiale. There are 2 weak spots in the capsule of the cubital articulation: They are the sacciform recessus and the posterio-superior area of the capsule.
In the region of the cubital articulation, there is a network formed bya. Recurrens ulnaris (a. Ulnaris), the branches of which anastomoses with a. Collateralis ulnares superior et inferior (a. Brachialis). A. Recurrens radialis forms ananstomoses with a. Collateralis radialis et media (a. Profunda brachii).
ANTEBRACHIAL REGION
The antebrachial region is limited: superiorly by 2 transverse fingers below the line, which joins the medial and lateral epicondyle of the humerus, inferiorly by the line that joins the styloideus process of the radius and ulna.
The layer-by-layer composition of this region: skin, subcutaneous fatty layer, superficial and the proper fascias.
Through the subcutaneous fatty layer passes v. Cephalica et n. Cutaneous antebrachii lateralis; v. Basilica et n. cutaneous antebrachii medialis.
The muscles of the anterior surface of the forearm are reapresented by four layers:
1 layer- m. Palmares longus, m. Pronator teres, m. Brachioradialis, m. Flexor carpi radialis. M. Flexor carpi ulnaris.
2 layer- m. Flexor digitorum superficialis
3 layer- m. Flexor digitorum profundus et m. Pollicis longus
4 layer- m. Pronator quadratus.
In the lower third of the forearm is located the cellulose space of Pirogov, which is limited by the 3rd and 4th layers of muscles.
A. Brachialis in the cubital fossa gets divided into two branches: a. Ulnaris, a.radialis
A. ULNARIS is the largest branch of a. Brachialis. In the upper third of the forearm the artery passes under m. Pronator teres. In the middle and lower thirds of the forearm a. Ulnaris and n. ulnaris pass in between m. Flexor digitorum superficialis and m. Flexor carpi ulnaris (forms the medial neuro-vascular bundle of the forearm). In the radial side of the pisform bone, a. Ulnaris and n. ulnaris passes into the canalis carpi ularis (interaponeurotic space)
The brances of a. Ulnaris:
1. a. Recurrens ulnaris
2. a. Interrossea communis goes to interosseal membrane and gets divided into 2 branches:
a) a. Interossea anterior passes along the anterior surface of the interosseal membrane, and gives a. Mediana.
b) a. Interossea posterior passes along the posterior surface of the forearm and together with the deep ramus of n. radialis forms the posterior neuro-vascular bundle of the forearm.
3. Ramus carpeus palmaris
4. Ramus carpeus dorsalis
5. Ramus palmaris profundus of a. Ulnaris forms anastomoses with a. Radialis and forms arcus palmaris profundus, which is located in between the tendon of m. Flexor digitorum and metacarpal bone.
A.v.v. Mediana and n. medianus forms the middle neuro-vascular bundle of the forearm. The middle third of the forearm passes between m. Flexor digitorum superficialis et profundus. In the lower thirds of the forearm, they pass between m. Flexor digitorum superficialis and m. Flexor carpi radialis.
A.v.v. interossea anterior and n. interosssea anterior forms the deep neuro vascular bundle of the forearm.
A. RADIALIS goes into the radia sulcus along with n. radialis in between m. Brachioradialis and flexor carpi radialis.
The branches of a. Radialis:
1. a. Recurrens radialis
2. Rami musculares (to the adjacent muscles)
3. Ramus carpeus
4. Ramus palmaris superficialis of a. Radialis anastomoses with ramus carpeus palmaris a. Ulnaris and forms arcus palmaris superficialis ( which is located in between the tendons of the flexor digitorum and the aponeurosis palmaris).
5. Ramus carpeus dorsalis
6. a. Metacarpea dorsalis prima
7. a. Princeps pollicis
REGIO PALMA MANUS
The layer-by-layer structure of the region: skin, subcutaneous fatty tissue, superficial fascia, proper fascia (aponeurosis palmaris). The proper fascia gives a septum, which divides Palma manus into 3 fascial beds: lateral (thenar), medial (hypothenar) and middle. In each of these beds are located the muscles, tendons, vessels, nerves, cellulose spaces. The muscles of the thenar are m. Abductor pollicis brevis, m. Opponens pollicis, m. Flexor pollicis brevis. Muscles of the hypothenar are mm. Flexor abductor opponens digiti minimi.
There are 4 cellulose spaces in the palm, where in case of pus formation, phlegmons are formed and are referred to as: thenar, hypothenar, sub aponeurotic, subtendonic, comissural.
Synovial vaginas of the tendons of the flexors of the fingers have a speciality. The synovial vagina of the first and the fifth fingers start from the region of the base of the distal phalange and ends in the lower third of the forearm in the cellulose space of Pirogov, forming the radial and ulnar synovial bags. The synovial vagina of the 2, 3, 4 th fingers starts from the region of the base of the distal phalange and ends in the region of the head of the carpal bones.
The wrist is supplied by the superficial and the deep arterial arches.
The palmar side of the wrist and the fingers are innervated by n. medianus et n. ulnaris. The dorsal side of the wrist and the fingers are innervated by n. radialis and n. ulnaris.
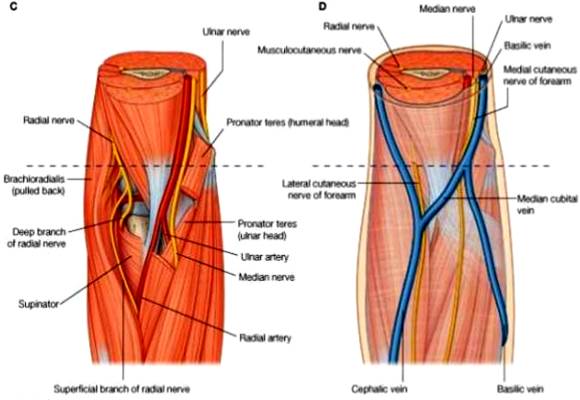
Fig. 8. FOSSA CUBITI, REGIO ANTEBRACHII, REGIO PALMA MANUS.
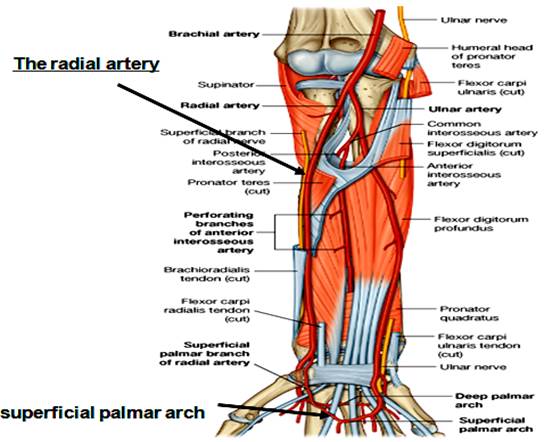
Fig. 9. FOSSA CUBITI, REGIO ANTEBRACHII, REGIO PALMA MANUS.
ЗАНЯТИЕ № 3.
FOSSA CUBITI.
Fossa cubiti ограничена сверху латерально m. brachioradialis, сверху медиально m. biceps brachii, снизу латерально m. brachioradialis, снизу медиально m. pronator teres. Слои области: кожа, подкожная жировая клетчатка, собственная фасция, окружающая сосудисто-нервные пучки и мышцы области.
В подкожной жировой клетчатке располагаются поверхностные вены и кожные нервы: латерально – v . cephalica et n. cutaneus antebrachii lateralis (выходит в fossa cubiti между m. biceps brachii et m. brachialis); медиально – v. basilica et n. cutaneus antebrachii medialis. Вены образуют между собой 2 вида анастомозов.
1. «И»- образный (v. mediana cubiti);
2. «М» - образный (v. mediana cephalica, v. mediana basilaca et v. mediana antebrachii).
В fossa cubiti проходит 2 сосудисто-нервных пучка. Латеральный - n. radialis et a.v. collateralis radialis. Нерв выходит в fossa cubiti между m. brachialis et m. brachioradialis. Он разделяется на ramus superficialis n.radialis, идущий на переднюю поверхность предплечья и ramus profundus n.radialis идущий через canalis supinatorius на заднюю поверхность предплечья. Медиальный сосудисто-нервный пучок образован a.v.v. brachialis et n. medianus. Артерия проходит медиально от m. biceps brachii, нерв медиально от артерии на 0,5-1 см.
На задней поверхности локтевой области располагается canalis osteo-fibrosus, который образован epicondilus medialis os brachii et olecranon os ulna. В канале проходит n. ulnaris et a.v. collateralis ulnaris superior.
ARTICULATIO CUBITI.
Articulatio cubiti образован тремя костями: os humeri, os ulna, os radii.
Сустав укреплен тремя связками: ligamentum anulare radii, ligamentum collaterale ulnare, ligamentum collaterale radiale. В капсуле аrticulatio cubiti выделяют два слабых места – это recessus sacciformis, и задне-верхний отдел капсулы.
В области аrticulatio cubiti имеется rete articulare cubiti, которая образована а. reccurens ulnaris (a. ulnaris), ветви которой анастомозируют с aa. collaterales ulnares superior et inferior (a. brachialis). A. reccurens radialis анастомозирует с a. collateralis radialis et media (a. profunda brachii).
REGIO ANTEBRACHII .
Границы области: сверху на 2 поперечных пальца ниже линии, соединяющей epicondilus lateralis et madialis os brachii, снизу – линия соединяющая processus styloideus os radii et ulna.
Послойное строение области: кожа, подкожная жировая клетчатка, поверхностная и собственная фасции.
В подкожной жировой клетчатке проходят v. cephalica et n. cutaneus antebrachii lateralis; v. basilica et n. cutaneus antebrachii medialis.
Мышцы передней поверхности предплечья представлены четырьмя слоями.
1 слой – m. palmaris longus, m. pronator teres, m. brachioradialis, m. flexor carpi radialis, m. flexor carpi ulnaris.
2 слой – m. flexor digitorum superficialis.
3 слой – m. flexor digitorum profundus et m. pollicis longus.
4 слой – m. pronator quadratus.
В нижней трети предплечья расположено клетчаточное пространство Пирогова, ограниченное 3 и 4 слоями мышц.
A. brachialis в fossa cubiti разделяется на две ветви: а. ulnaris et а. radialis.
А. ULNARIS более крупная ветвь а. brachialis. В верхней трети предплечья она проходит под m. pronator teres. В средней и нижней трети предплечья а. ulnaris проходит с n. ulnaris между m. flexor digitorum superficialis и m. flexor carpi ulnaris (образует медиальный сосудисто-нервный пучок предплечья). У лучевой стороны os pisiformis a. ulnaris et n. ulnaris проходит в canalis carpi ulnaris (spatium interaponeuroticum).
Ветви a. ulnaris:
1. A. reccurens ulnaris,
2. A. interossea communis, идет к membrana interossea и делится две ветви: а) а. interossea anterior проходит по передней поверхности membrana interossea, отдает а. mediana
б) а. interossea posterior проходит на заднюю поверхность antebrachii и вместе с ramus profundus n. radialis образует задний сосудисто-нервный пучок antebrachii.
3. Ramus carpeus palmaris.
4. Ramus carpeus dorsalis.
5. Ramus palmaris profundus a. ulanaris анастомозирует с a. radialis и образует arcus palmaris profundus, которая располагается между tendo m. flexor digitorum и os metacarpi.
A.v.v. mediana et n. medianus образуют срединный сосудисто-нервный пучок antebrachii. В средней трети предплечья они проходят между m. flexor digitorum superficialis et profundus. В нижней трети предплечья они проходят между m. flexor digitorum superficialis et m. flexor carpi radialis.
A.v.v. interossea anterior et n. interossea anterior образуют глубокий сосудисто-нервный пучок предплечья.
А . RADIALIS идет в sulcus radialis с r. superficialis n. radialis между m. brachioradialis et flexor carpi radialis.
Ветви a. radialis:
1. А. recurrens radialis.
2. Rami musculares - к окружающим мышцам.
3. Ramus carpeus.
4. Ramus palmaris superficialis a. radialis анастомозирует с ramus carpeus palmaris a. ulnaris и образует arcus palmaris superficialis (расположена между tendo flexor digitorum et aponeurosis palmaris).
5. Ramus carpeus dorsalis.
6. A. metacarpea dorsalis prima
7. A. princeps pollicis
REGIO PALMA MANUS.
Послойное строение области: кожа, подкожная клетчатка, fascia superficialis, fascia propria (aponeurosis palmaris). Fascia propria отдает перегородки, которые разделяют palma manus на 3 фасциальных ложа: латеральное (thenar), медиальное (hypotenar), срединное. В каждом фасциальном ложе располагаются мышцы, сухожилия, сосуды, нервы, клетчаточные пространства. К мышцам thenar относятся: m. abductor pollicis brevis, m. opponens pollicis, m. flexor pollicis brevis. К мышцам hypotenar относятся mm. Flexor, abductor, opponens digiti minimi.
На ладони выделяют 4 клетчаточных пространства, в которых при нагноительных процессах образуются одноименные флегмоны: thenar, hypotenar, подапоневротическая, подсухожильная, комиссуральная.
Синовиальные влагалища сухожилий сгибателей пальцев имеют особенности. Синовиальные влагалища 1 и 5 пальцев кисти начинаются в области основания ногтевой фаланги и заканчиваются в нижней трети предплечья в клетчаточном пространстве Пирогова, образуя локтевой и лучевой синовиальные мешки. Синовиальные влагалища 2, 3, 4 пальцев кисти начинаются в области основания ногтевых фаланг и заканчиваются на кисти в области головок пястных костей.
Кровоснабжение кисти осуществляется поверхностной и глубокой артериальными дугами. Иннервация ладонной поверхности кисти и пальцев – n. medianus et n. ulnaris. Иннервация тыльной поверхности кисти и пальцев – n. radialis et n. ulnaris.
LECTURE 4
GLUTEAL REGION
The gluteal region is limited: superiorly by crista iliaca, inferiorly by sulcus gluteus, medially by the middle area od the sacral bone, laterally by the line that joins the spina iliaca anterior superior to the trochanter major of the femur.
The layer-by-layer composition of the region: skin, subcutaneous fatty layer, superficial and proper fascias (fascia glutea).
The muscles of the gluteal region are located in three layers:
1 layer- m. Gluteus maximus, 1/3 of m. Gluteus medius
2 layer- 2/3 of m. Gluteus medius, m. Piriformis, m. Gemilli, m. Obturatorius internus, m. Quadratus femoris,
3 layer- m. Gluteus minimus, m. Obturatorius externus.
M. piriformis divides the major ischiadic foramen into 2: foramen suprapiriformis and foramen infrapiriformis. Foramen suprapiriformis is limited superiorly by m. Gluteus medius and inferiorly by m. Piriformis. Through the foramen suprapiriformis passes the superior neuro-vascular bundle a.v.n. gluteus superior. Foramen infrapiriformis is limited superiorly by m. Piriformis and inferiorly by m. Gemelli. Through the foramen infrapiriformis passes three neuro-vascular bundles. Inferiorly - a.v.n. gluteus inferior; inferio-medially - a.v. pudenda interna, n. pudendus; inferio-laterally- n. ischiadicus, a.v. comitans n. ischaidicus, n. cutaneous femoris posterior.
ARTICULATIO COXAE
The hip joint is formed by the facies lunata os the acetabulum of the pelvic bone and the femoral head.
The articulation consists of two intra- articular ligaments: lig. Transversum acetabuli and lig. Capitis femoris.
The external ligaments of the joint, which corresponds to the three axes of rotation are: 3 longitudinal (lig. Iliofemorale, pubofemorale and lig. Ischiofemorale) and circular (orbicular zone).
FEMORAL REGION
The femoral region is limited superiorly in the front by inguinal ligament, posteriorly above by the gluteal fold: iferiorly by the circular line which passes at the level two transverse fingers above the patella.
The layer-by layer structure of this region: skin, subcutaneous fatty layer, superficial fascia, the proper fascia (lata fascia). In the subcutaneous fatty layer arre located: v. Saphena magna, n. cutaneous femoris anterior (n. femoralis), n. cutaneous femoralis medialis (n. obturatorius ), n. cutaneous femoris lateralis (plexus lumbalis), ramus femoralis (n. genitofemoralis), n. cutaneous femoris posterior (plexus sacralis).
ANTERIOR FEMORAL REGION:
The main neuro-vascular bundle of the region in the upper thirds of the femur is a.v. femoralis et n. femoralis. In between the inguinal ligament and the bones of the pelvis is located the lacuno musculorum and lacuna vasorum. Lacuna musculorum is limited superiorly by the inguinal ligament, inferiorly by the ileal bone, medially by the iloiopectineal arch. Lacuno vasorum is limited superiorly by the inguinal ligament, laterally by the iliopectineal arch, inferiorly by lig. Pectineale, medially by lig. Lacunare. Through the lacuna vasorum passes a.v. femoralis.
FEMORAL CANAL:
In the medial corner of the lacuna vasorum is located the cellulose, through which protrudes the femoral hernia. In this case, a femoral canal of length 1-2 cms is formed. The femoral canal has an internal ring, external ring and a wall.
The internal ring is limited: superiorly by inguinal ligament, laterally by v. Femoralis, inferiorly by lig. Pectineale, medially by lig. Lacunare.
The external ring- this is the hiatus saphenus on the superficial lamina of the fascia lata, through which normally passes v. Saphena magna
The walls of the canal are formed laterally by v. Femoralis, anteriorly and posteriorly by superficial lamina and deep lamia of the fascia lata.
FEMORAL TRIANGLE:
The femoral triangle is limited superiorly by lig. Inguinale, laterally by m. Saratorius, medially by m.adductor longus. The fundus of the triangle is covered by two muscles: m. Pectineus and m. Iliopsoas.
In the triangle, below the inguinal ligament in the upper third of the femur passes: v. Femoralis medially, a. Femoralis laterally, and n. femoralis more laterally.
In the lower thirds of the femur is located medially n. saphenus, laterally- a. Femoralis and more laterally and deeply- v. Femoralis.
ADDUCTOR CANAL (GUNTER’S):
In the lower third of the femur, n. saphenus, a. Femoralis and v. Femoralis enter the adductor canal through its upper foramen. The canal is limited laterally by vastus medialis of m. Quadriceps femoralis, medially by m. Adductor magnus, anteriorly by lamina vasoadductoria, on which lies m. Sartorius. Through the anterior foramen of the canal passes n. saphenus and a.v. genus descendens (a.v. femoralis). Through the inferior foramen of the canal in the popliteal fossa passes the a.v. poplitea (a.v. femoralis).
A. FEMORALIS is the continuation of a.iliaca externa. On the femur it passes through the sulcus ileopectineus, and then through the sulcus femoris anterior and then through the adductor canal enters into the popliteal fossa, where the a. Poplitea is located. To stop the bleeding from a. Femoralis, we can apply pressure under lig. Inguinale to the pubic bone.
The branches of a. Femoralis:
A) Superficial (subcutaneous):
1. a. Epigastrica superficialis
2. a. Circumflexa ileum superficialis.
3. a. Pudenda externae
B) Deep (primary):
4. a. Profunda femoris
Branches of a. Profunda femoris:
a) a. Circumflexa femoris medialis
b) a. Circumflexa femoris lateralis , divides into ramus ascendens and ramus descendens.
c) aa. Perforantes
5. r. Musculares
6. a. Genus descendens.
POSTERIOR FEMORAL REGION
The primary neuro vascular bundles of the region are n. ischiadicus and a.v. comitans n. ischiadici. N. ischiadicus is located between m. Semitendinosus, m. Semi membranosus and m. Biceps femoris. N. ischiadicus in the lower third of the femur divides into n.tibalis and n. peroneus communis.
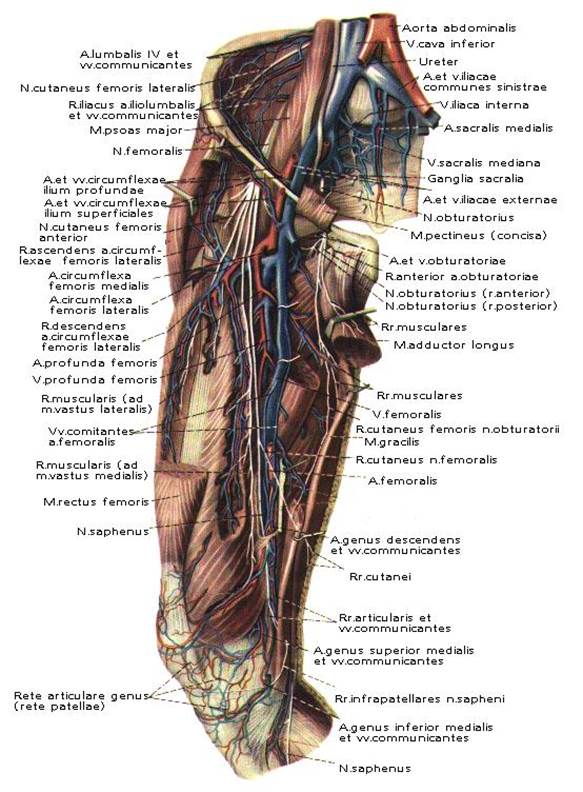
Fig. 10. Topography of regio femoris anterior.
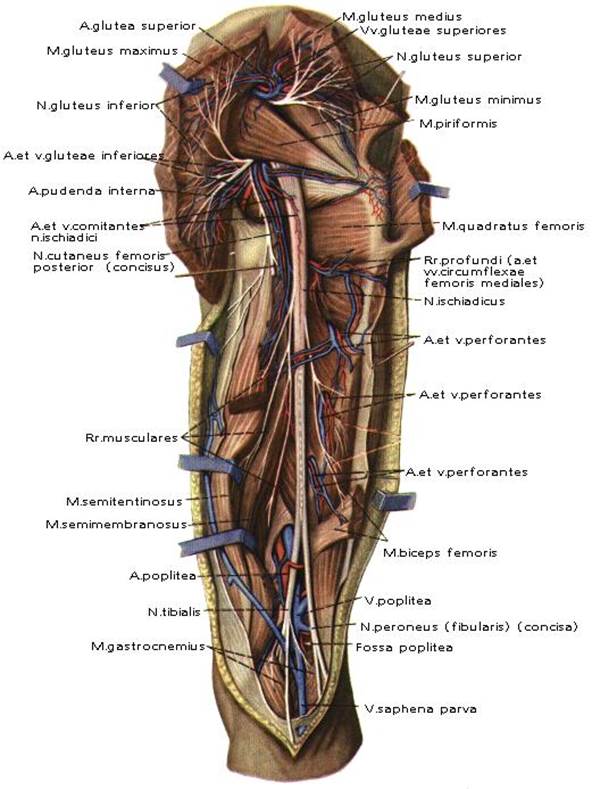
Fig.11. Topography of regio femoris posterior.
ЗАНЯТИЕ № 4.
REGIO GLUTEA.
Regio glutea ограничена: сверху – crista iliaca, снизу – sulcus gluteus, медиально – середина os sacrum, латерально – линия, идущая от spina iliaca anterior superior до trochanter major os femur.
Послойное строение области: кожа, подкожная жировая клетчатка, поверхностная, собственная фасция (fascia glutea).
Мышцы regio glutea расположены в три слоя:
1 слой – m. gluteus maximus, 1/3 m. gluteus medius;
2 слой – 2/3 m. gluteus medius, m. piriformis, m. gemelli, m. obturatorius internus, m. quadratus femoris;
3 слой – m. gluteus minimus, m. obturatorius externus.
M. piriformis разделяет foramen ishiadicum majus на два отверстия: foramen suprapiriformis и foramen infrapiriformis. Foramen suprapiriformis ограничено сверху m. gluteus medius снизу m. piriformis. Через foramen suprapiriformis проходит верхний сосудисто-нервный пучок a.v.n. gluteus superior. Foramen infrapiriformis ограничено сверху m. piriformis снизу m. gemelli. Через foramen infrapiriformis проходит три сосудисто-нервных пучка. Нижний - a.v.n. gluteus inferior; нижне-медиальный – a.v. pudenda interna, n. pudendus; нижне-латеральный – n. ishiadicus, a.v. comitans n. ishiadici, n. cutaneus femoris posterior.
ARTICULACIO COXAE.
Тазобедренный сустав, articulatio coxae, образован facies lunata acetabulum тазовой кости и capitis femoris.
Articulatio coxae имеет две внутрисуставные связки: lig. transversum acetabuli и lig. capitis femoris.
Соответственно трем основным осям вращения располагаются наружные связки сустава: три продольные (ligg. iliofemorale, pubofemorale et ischiofemorale) и круговая (zona orbicularis).
REGIO FEMORIS .
Regio femoris ограничена сверху спереди ligamentum inguinale, сзади сверху ягодичной складкой; снизу циркулярной линией, проходящей на два поперечных пальца выше patellae.
Послойное строение области: кожа, подкожная жировая клетчатка, поверхностная фасция, собственная фасция (fascia lata). В подкожной жировой клетчатке располагаются: v. saphena magna, n. cutaneus femoris anterior (n. femoralis), n. cutaneus femoris medialis (n. obturatorius), n. cutaneus femoris lateralis (plexus lumbalis), ramus femoralis (n. genitofemoralis), n. cutaneus femoris posterior (plexus sacralis).
Regio femoris anterior.
Основным сосудисто-нервным пучком regio femoris anterior в верхней трети бедра является a.v. femoralis et n. femoralis. Между ligamentum inguinale и костями таза располагаются lacuna musculorum et lacuna vasorum. Lacuna musculorum ограничена сверху ligamentum inguinale, снизу os ilium, медиально arcus iliopectineus. Lacuna vasorum ограничена сверху ligamentum inguinale, латерально arcus iliopectineus, снизу lig. pectineale, медиально lig. lacunare. Через lacuna musculorum проходит m. iliopsoas et n. femoralis. Через lacuna vasorum проходит a. et. v. femoralis.
Canalis femoralis .
В медиальном углу lacuna vasorum располагается клетчатка, через которую могут выходить бедренные грыжи. При этом в патологии, образуется canalis femoralis длиной 1-2 см. Canalis femoralis имеет внутреннее кольцо, наружное кольцо и стенки.
Внутреннее кольцо ограничено: сверху ligamentum inguinale, латерально v.femoralis, снизу lig. pectineale, медиально lig. lacunare.
Наружное кольцо – это hiatus saphenus в lamina superficialis fascia lata, через которое в норме проходит v.saphena magna.
Стенки канала образованы: латерально v. femoralis, спереди и сзади lamina superficialis et profunda fascia lata.
Trigonum femorale.
Trigonum femorale ограничен сверху – lig. inguinale, латерально – m. sartorius, медиально – m. adductor longus. Дно trigonum femorale покрывают две мышцы – m. pectineus et m. iliopsoas.
В trigonum femorale проходят под lig. inguinale в верхней трети бедра медиально – v. femoralis, латерально – a. femoralis, еще латеральнее – n. femoralis.
В нижней трети бедра медиально располагается n. saphenus, латерально – a. femoralis еще латеральнее и глубже – v. femoralis.
С analis adductorius ( Gunter ` s ).
В нижней трети бедра n. saphenus, a. femoralis и v. femoralis через верхнее отверстие идут в canalis adductorius. Canalis adductorius ограничен латерально – vastus medialis m. guadriceps femoris, медиально – m. adductor magnus, спереди – lamina vastoadductoria, на которой лежит m. sartorius. Через переднее отверстие канала проходит n. saphenus и a.v. genus descendens (a.v. femoralis). Через нижнее отверстие канала в fossa poplitea выходит a.v. poplitea (a.v. femoralis).
А. femoralis представляет продолжение a. iliaca externa. На бедре проходит в sulcus iliopectineus, затем в sulcus femoralis anterior, и через canalis adductorius идет в fossa poplitea, где продолжается в а. poplitea.. Для остановки кровотечения a. femoralis прижимают под lig. inguinale к os pubis.
Ветви а. femoralis:
А) Поверхностные (подкожные).
1. A. epigastrica superficialis.
2. A. circumflexa ilium superficialis.
3. Aa. pudendae externae.
В) Глубокие (основные).
4. A. profunda femoris.
Ветви а. profunda femoris:
а) а. circumflexa femoris medialis;
б) а. circumflexa femoris lateralis, делится на ramus ascedens и ramus descedens;
в) aa. perforantes.
5. Rami musculares.
6. A. genus descedens.
Regio femoris posterior.
Основным сосудисто-нервным пучком region femoris posterior является n. ischiadicus et a.v. comitans n. ischiadici. N. ischiadicus располагается между m. semitandinosus, m. semimembranosus et m. biceps femoris. N. ischiadicus в нижней трети бедра делится на n. tibialis et n. peroneus communis.
LECTURE 5
ARTICULATIO GENU
The knee joint is the biggest and complexest of all the joints. It is formed by the femur, the tibia, the patella. On the superior articular surface of the tibia there is intra-articular cartilage or meniscus lateral and medial meniscus.
Anteriorly, the meniscus is connected by the intra-articular lig. Transversum genus. And also to the group of intra-articular ligaments are included the ligg. Cruciatum anterius et posterius. To the extra- articular ligaments includes: lig. Patella, lig. Collaterale tibiale, lig. Collaterale fibulare; posteriorly: lig. Popliteum arcuatum and lig. Popliteum obliquum.
In the region of the knee joint, there are numerous bursas that communicate and those that do not communicate with the joint cavity. They are bursa suprapatellaris, bursa prepatellaris subcutanea, bursa subfascialis prepatellaris, bursa subtendinea prepatellaris, and bursa infrapatellaris profunda.
The knee joint is supplied by the articular network, which is formed by aa. Genus superiores mediales et laterale, aa. Genus inferiores mediales et laterales, a. Genus media (a. Poplitea), a. Genus descendens (a. Femoralis), aa. Recurrentes tibiales anterior et posterior (a. Tibiales anterior).
FOSSA POPLITEA
The popliteal fossa is limited: medially above by m. Semitendinosus et m. Semimembranosus, laterally above by m. Biceps femoris, inferiorly by m. Gastrocnemius (caput laterale et caput mediale).
The layer-by layer structure of the region: skin, subcutaneous fatty layer, superficial fascia and the proper fascia (popliteal fascia). In the subcutaneous fatty layer passes: v. Saphena magna and n. saphenus medially, v. Saphena parva et n. cutaneous surae medialis laterally. N. cutaneous femoris posterior also pass through the sub cutaneous fatty layer.
The primary neuro-vascular bundle consists of n. tibialis (n. ischiadicus) superficially and laterally; v.poplitea deeply and medially. Laterally along the tendon of m. Biceps femoris passes the n. perneous communis (n. ischiadicus).
A. poplitea is the continuation of a. Femoralis. In the popliteal fossa, a. Poplitea is located on the bone itself, where it can be pressurised to stop bleeding.
Branches of a. Poplitea:
A) Which branch in the popliteal fossa:
1. Aa. Genus superiores lateralis et mediales.
2. Aa. Genus inferiores lateralis et mediales
3. Aa. Genus media
B) Terminal branches:
4. A. Tibiales anterior
5. A. Tibiales posterior
REGIO CRURIS
The crural region is limited superiorly by a horizontal line which passes through the tibial tuberositas and fibular capitulum; inferiorly by a horizontal line which passes through the lateral malleolus of the fibula and medial malleolus of the tibia.
The layer-by layer composition of the region: skin, subcutaneous fatty layer, superficial fascia, proper fascia (crural fascia).Through the subcutaneous fatty layer passes: v. Saphena magna and n. saphenus medially, v.saphena parva and n. cutaneous surae medialis laterally. And also in the subcutaneous fatty layer passes thye n. cutaneous surae lateralis, which in the lower third of the thigh, along with n. cutaneous surae medialis n. suralis and n. peroneus superficialis (n. peroneus communis).
The proper fascia of the crural region forms a septum, which divides the region into three fascial beds. Large neurovascular bundles pass through each of these fascial beds.
The anterior neurovascular bundle consists of a.v. tibialis anterior and n. peroneus profundus. A. Tibialis anterior (a. Poplitea) in the upper thirds of the thigh, passes between m. Tibialis anterior and m. Extensor digitorum longus, and still below lies between m. Tibialis anterior and m. Extensor hallucis longus. In the upper part, the nerve is located laterally and in the lower parts is located medial to the artery.
Branches of a. Tibialis anterior:
1. A. Recurrens tibiales posterior
2. A. Recurrens tibiales anterior.
3. Aa. Malleolares anteriores mediales et lateralis, which take part in the formation of the medial and the lateral malleolar network ( rete malleolare mediale et laterale).
In the anterio- lateral bed there are two canals:
1. Superior musculoperoneal canal is formed by the fibula and m. Peroneus longus. N. peroneus superficialis passes throught the canal.
2. Inferior musculoperoneal canal is formed by the fibula and m. Flexor hallucis longus. A.v. peronea passes through the canal.
The posterior neuro-vascular bundle consists of a.v. tibiales posterior and n. tibialis. A. Tibiales posterior (a. Poplitea) passes through the cruropopliteal canal. In the upper parts the foramen is limited by m. Soleus et caput laterale et mediale m. Gastrocnemius. The cruropopliteal canal is limited anteriorly by m. Tibiales posterior, and posteriorly by m. Soleus, laterally by m. Flexor hallucis longus, medially by m. Flexor digitorum longus.
The branches of a. Tibiales posterior:
1. A. Plantaris medialis.
2. A. Plantaris lateralis.
3. A. Peronea (fibularis)
REGIO MALLEOLUS MEDIALIS
The borders of the region correspond to that of the borders of malleolus medialis and Achille’s tendons. Through the subcutaneous fatty layer passes n. saphena magna and n. Saphenus. The malleolar canal is limited by the medial malleolus, retinaculum flexorum and the Achille’s tendon. Through the canal passes the tendons of m. Flexor digitorum longus, m. Tibiales posterior, m. Flexor hallucis longus, a.v.v. tibiales posterior and n. tibialis. The neuro-vascular bundle gets divided into 2 (a.v.v.n. plantares lateralis et mediales).
REGIO PEDIS
DORSUM PEDIS:
In the subcutaneous fatty layer is located the venous network of the dorsal pedis, and v. Saphena magna starts medially and v. Saphena parva starts laterally. The skin i the region is innervated by n. saphenus, n. cutaneus dorsalis pedis lateralis (n. suralis), n. peroneus superficialis et profundus.
The primary artery of the region is a. Dorsalis pedis.
Branches of a. Dorsalis pedis:
1. Aa. Tarseae mediales
2. A. Tarsea lateralis
3. A. Arcuata. From this artery branches out three aa. Metatarsea dorsales, each of which gets divided into two aa. Digitales dorsales communis, which continues as aa. Digitales dorsales propria;
4. A. Metatarsea dorsalis prima
5. Ramus plantaris profundus.
PLANTA PEDIS
Regio planta pedis is supplied by aa. Plantares mediales et laterales. A. Plantaris medialis is located in the sulcus plantaris medialis. The larger a. Plantaris lateralis passes into the sulcus plantaris lateralis and takes part in the formation of arcus plantaris.
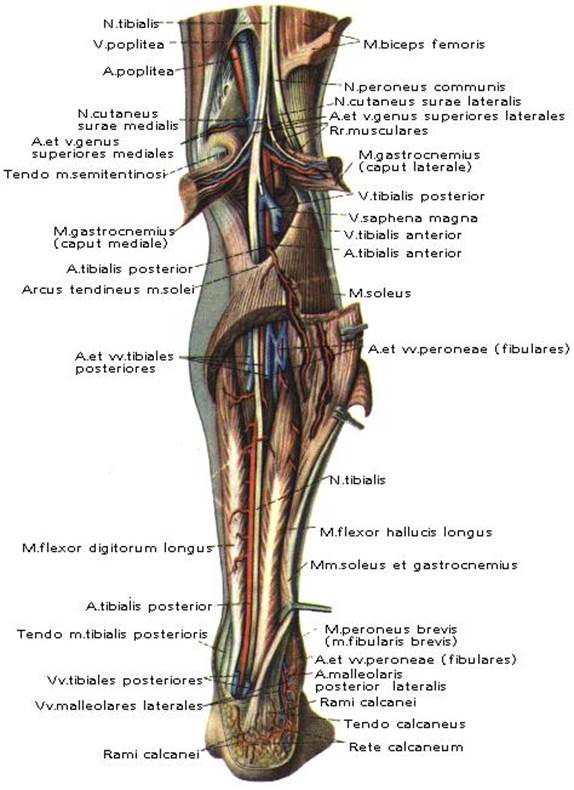
Fig. 12. Topography of region fossa poplitea et regio cruris posterior.
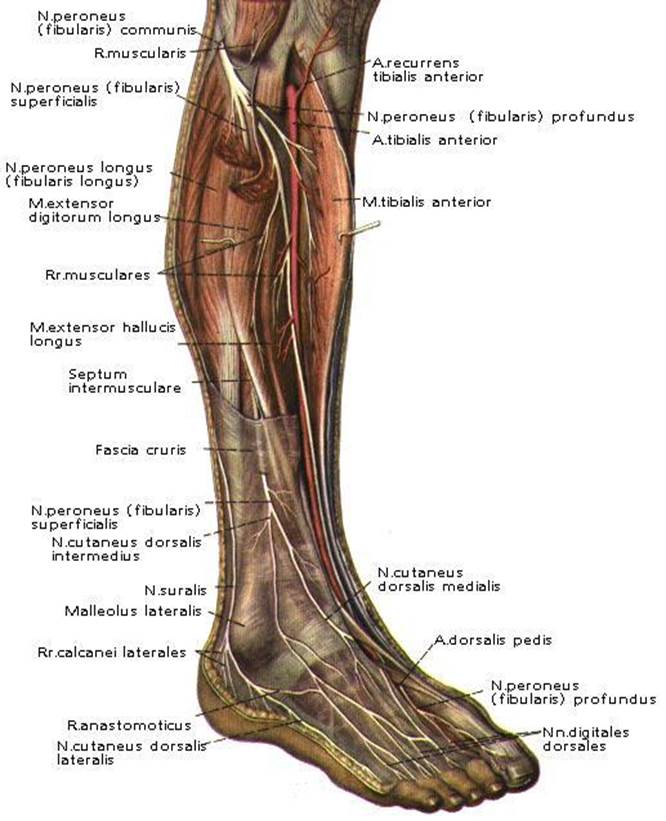
Fig. 13. Topography of region cruris anterior.
ЗАНЯТИЕ № 5.
ТОПОГРАФИЯ ARTICULATIO GENU, FOSSA POPLITEA, REGIO CRURIS, REGIO MALLEOLUS MEDIALIS, REGIO PEDIS.
ARTICULATIO GENU .
Art. genu, является самым большим и сложным из всех суставов. В его образовании принимают участие: os femor, os tibia, patella. На facies articularis superior os tibia имеются внутрисуставные хрящи, или мениски – meniscus lateralis et medialis. Спереди мениски соединены внутрисуставной связкой lig.
transversum genus. Также к внутрисуставным связкам относятся ligg. cruciatum anterius et posterius. К внесуставным связкам относятся: передние – lig. patellae, lig. collaterale tibiale, lig. collaterale fibulare; задние – lig. рорliteum arcuatum и lig. popliteum obliquum.
В region articulatio genu имеется ряд сумок сообщающихся и не сообщающихся с полостью сустава. Это bursa suprapatellaris, bursa prepatellaris subcutanea, bursa subfascialis prepatellaris, bursa subtendinea prepatellaris, bursa infrapatellaris profunda.
Art. genu кровоснабжается rete articulare, которая образована aa. genus
superiores medialis et lateralis, aa. genus inferiores medialis et lateralis, a. genus media (a. poplitea), a. genus descendens (a. femoralis), aa. recurrentes tibiales anterior et posterior (a. tibialis anterior).
FOSSA POPLITEA.
Fossa poplitea ограничена сверху медиально – m. semitendinosus et m. semimembranosus, сверху латерально – m. biceps femoris, снизу – m. gastrocnemius (caput laterale et caput mediale).
Послойное строение – кожа, подкожная жировая клетчатка, поверхностная фасция, собственная фасция (fascia poplitea). В подкожной жировой клетчатке проходят: медиально – v. saphena magna et n. saphenus, латерально – v. saphena parva et n. cutaneus surae medialis. Также в подкожной жировой клетчатке проходят n. cutaneus surae lateralis et n. cutaneus femoris posterior.
Основным сосудисто-нервным пучком является: поверхностно латерально – n. tibialis (n. ischiadicus); глубже, медиально – v. poplitea; еще глубже и медиально – a. poplitea. Латерально, вдоль tendo m. biceps femoris проходит n. peroneus communis (n. ischiadicus).
A. poplitea, продолжение a. femoralis. В fossa poplitea a. poplitea располагается на самой кости, где ее можно пережать.
Ветви a . poplitea :
А) Отходящие в fossa poplitea.
1. Aa. genus superiores lateralis et medialis.
2. Aa. genus inferiores lateralis et medialis.
3. A. genus media.
В) Конечные ветви.
4. A. tibialis anterior.
5. A. tibialis posterior.
REGIO CRURIS.
Regio cruris ограничена сверху горизонтальной линией, проходящей через tuberositas tibia et capitulum fibula; снизу горизонтальной линией, проходящей через malleolus lateralis os fibula et medialis os tibia.
Послойное строение – кожа, подкожная жировая клетчатка, поверхностная фасция, собственная фасция (fascia cruris). В подкожной жировой клетчатке проходят: медиально – v. saphena magna et n. saphenus, латерально – v. saphena parva et n. cutaneus surae medialis. Также в подкожной жировой клетчатке проходят n. cutaneus surae lateralis, образующий в нижней трети голени вместе с n. cutaneus surae medialis n. suralis et n. peroneus superficialis (n. peroneus communis).
Собственная фасция голени дает перегородки, которые разделяют голень на три фасциальных ложа. В каждом фасциальном ложе проходят крупные сосудисто-нервные пучки.
Передний сосудисто-нервный пучок состоит из a.v. tibialis anterior et n. peroneus profundus. A. tibialis anterior (a. poplitea) в верхней трети голени, проходит между m. tibialis anterior и m. eхtensor digitorum longus, а ниже лежит между m. tibialis anterior и m. eхtensor halluсis longus. Вверху нерв расположен латерально, а внизу медиально артерии.
Ветви a . tibialis anterior :
1. A. reсurrens tibialis posterior.
2. A. reсurrens tibialis anterior.
3. Aa. malleolares anteriores medialis et lateralis, участвуют в образовании retе malleolaгe mediale et lateгale.
В передне-латеральном ложе голени имеется два канала.
Canalis musculoperoneus superior образован os fibula et m. peroneus longus. В нем проходит n. peroneus superficialis.
Canalis musculoperoneus inferior образован os fibula et m. flexor hallucis longus. В нем проходит a.v. peronea.
Задний сосудисто-нервный пучок состоит из a.v. tibialis posterior et n. tibialis. A. tibialis posterior (a.poplitea) идет в сanalis сruropopliteus. Верхнее отверстие канала ограничено m. soleus et capus laterale et mediale m. gastrocnemius. Canalis сruropopliteus ограничен спереди – m. tibialis posterior, сзади – m. soleus, латерально – m. fleхor halluсis longus, медиально – m. flexor digitorum longus.
REGIO MALLEOLUS MEDIALIS.
Границы области соответствуют malleolus medialis et tendo Achilii.
В подкожной жировой клетчатке проходит v. saphena magna et n. saphenus. Сanalis malleolaris ограничен malleolus medialis, retinaculum flexorum et tendo Achilii. В канале проходят tendo m. flexor digitorum longus, m. tibialis posterior, m. fleхor halluсis longus, a.v.v. tibialis posterior et n. tibialis. Сосудисто-нервный пучок разделяется на 2 сосудисто-нервных пучка (a.v.v.n. plantares lateralis et medialis).
REGIO PEDIS.
Dorsum pedis.
В подкожной жировой клетчатке располагается rete venosum dorsalis pedis, медиально начинается v. saphena magna, латерально начинается v. saphena parva. Кожа области иннервируется n. saphenus, n. cutaneus dorsalis pedis lateralis (n. suralis), n. peroneus superficialis et profundus.
Основная артерия regio dorsum pedis a. dorsalis pedis.
Ветви a. dorsalis pedis:
1.Aa. tarseae mediales;
2.A. tarsea lateralis;
3.A. arсuata. От нее отходят три aa. metatarseae dorsales разделяющиеся каждая на две aa. digitales dorsales communis, продолжающиеся в aa. digitales dorsales propria;
4. A. metatarsea dorsalis prima;
5. Ramus plantaris pгofundus.
Planta pedis.
Regio planta pedis кровоснабжают aa. plantaгes medialis et lateralis. А. plantaris medialis располагается в sulсus plantaгis media1is. Более кpупная a. plantaris lateralis идет в sulсus plantaris latera1is и участвует в образовании arcus plantaris.
LECTURE 6
OPERATIONS ON VESSELS
Operations on arterial, venous and lymphatic vessels are a large division of modern surgery.
Three basic kinds of operations are carried out on vessels: ligation, vascular suture and vascular plasty.
Bleeding is the basic and most common indication of operations on vessels. The following are classifications of bleeding:
1) On source-arterial,venous,arteriovenous and capillary (parenchymatous);
2) On direction of blood outcome-external and internal;
3) On time of occurrence-initial and secondary.
The arterial bleeding makes up majority of bleedings. According to the Second World War (1941-1945) more than 80% of all bleedings were connected with arterial trunk damages.
Damage of the main arteries includes two dangers for victims:
1) Lethal outcome in connection with bleeding;
2) Necrosis of the distal part of extremity due to failure of collateral arteries blood supply.
The main arteries are divided, the non dangerous for ligation (a.ulnaris, a.radialis, a.tibialis anterior et posterior) and dangerous for ligation (a.subclavia, a.axillaris, a.brachialis, a.femoralis, a.poplitea, a.carotis communis et interna). Angiorrhaphy or vascular plasty are more preferable to make on such arteries. The degree of danger during ligation of the main arteries varies a lot, it depends on the level of ligation and anatomic conditions of collateral blood supply development.
During ligation of dangerous arteries two ligatures impose and there is a cross vessel between them for desimpatisation of nerve adventicia, expansions of collaterals and collateral blood supply.
V.A. Oppel ligates the same vein for blood balance regulation.
It is necessary to apply a vessel suture for stopping bleeding from dangerous vessels. If the vascular suture cannot be made at once, it is possible to make a temporary repair with the help of a tube made from synthetic material (polychlorvinil, silicon) for 72 hours. Washed with a solution of heparinum the tube is inserted in distal and proximal ends of the vessel and is fixed by ligatures.
The approach on a blood vessel is usually carried out by level-by-level section of tissues on the projective lines.
Ligation of vessels is made on a wound and at a distance, from a distance to the place of vessel damage.
Indications of ligation of arteries on extension:
1) Impossibility of vessel ligation on a wound when the vessel lays in thickness of an inflammatory infiltrate;
2) Traumatic aneurysms;
3) Amputation of extremity at gangrene, anaerobic infection.
METHODS OF FINAL HEMOSTASIS
Ligating of vessels in a wound is the most reliable way of controlling bleeding. The central and peripheral ends of a bleeding vessel are picked up, grasped with haemostatic clamps and ligated.
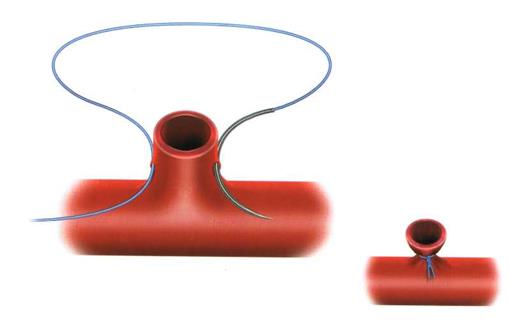

Fig. 14.Vascular ligations.
The central end is ligated twice during ligation of large arterial vessels. The central end is ligated by placing a suture for the second time in order to avoid slipping of ligatures and bleeding. Damaged vessels of small caliber can be grasped by haemostatic clamps and made vasoversion by rotary movements.
Sometimes if small wounds and damaged vessels of small caliber are present, it is possible to make tamponade of a wound. Frontal and back tamponade of a nose during nasal bleeding is a typical example of bleeding control.
VASCULAR SUTURE
The basic indication of angiorrhaphy is restoration of the main arteries’ permeability. There are manual vascular and mechanical vascular sutures.
The manual vascular suture may be lateral and circular. The mechanical vascular suture is placed by means of angiorrhaphy apparatus.
The demands of an angiorrhaphy are as follows:
1. Hermetism. It is reached by removal of vessel adventicia of 2-3 mm from the end, dense contact of intima, applying of close (through 1 mm) continuous blanked suture.
2. Prophylaxis of a thrombogenesis. It is reached by application of anticoagulants. The vascular suture should not break blood current (absence of narrowing and turbulence); suture material should be as small as possible in a lumen of vessel.
3. Prophylaxis of vessel lumen narrowing. It is reached by applying sutures which are stretched on the wall of the vessel, and the continuous vascular suture does not allow the wall of the vessel to constrict back to its former size.
Vascular sutures are placed manually with the help of atraumatic needles. A mechanical vascular suture is perfect and does not narrow vessel’s lumen but its used only during planned operations and the vessel's diameter must be more than 2,5 mm.
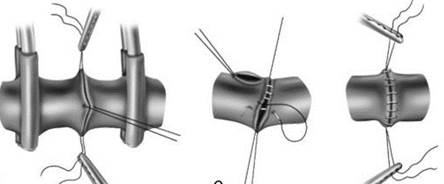
Fig. 15. Vascular sutures.
VASCULAR SUTURE BY CARREL
1. Approach to a vessel. A projective line is used for approaching a vessel. Approach includes level-by-level section of tissues on a line or at a distance of 1-2 cm from it: skin, hypodermic fatty tissue, superficial fascia, own fascia (forming fascial cover).
2. Mobilization. It is rising of a vessel and its accompanying vessels and nerves from a fascial bedsore. This stage also includes applying of Hepfner’s artery forceps at a distance of 1-2 cm from the ends of a vessel.
3. Angiorrhaphy. Excision of a vessel's damaged ends and removal of 2-3mm adventitia. The ends of the vessel are fixed by applying 3 sutures by Carrel. The vessel is sutured between fixating sutures by a continuous blanket suture of 1 mm using one of the strings from guy suture.
4. Level-by-level suturing of a wound.
VASCULAR PLASTY
When there is a big defect present transplantats from biological material is carried out. Autoveins are usually used (v.saphena magna, v.basilica).
Auto- and allotransplants of arteries and veins are used as transplants in vessel surgery; isotransplants made from synthetic materials are used. Reconstruction is made by applying an anastomosis of end-to-end or transplants suturing.
STENTING OPERATIONS
Heart surgery using stents is an indispensable and lifesaving surgical procedure mostly used when the patient has severe heart blockage, risk of a heart attack or arterial blockage.
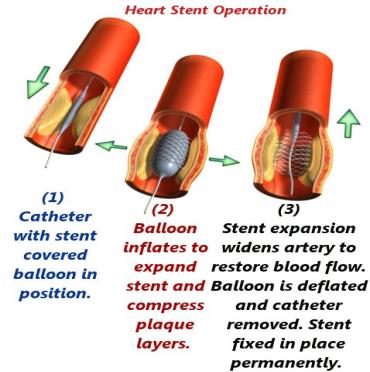
Fig. 16. Heart Stent Operation
ЗАНЯТИЕ № 6.
ОПЕРАЦИИ НА СОСУДАХ.
Операции на артериальных, венозных и лимфатических сосудах составляют крупный раздел современной хирургии.
На сосудах выполняют 3 основных вида операций: перевязку, сосудистый шов и сосудистую пластику.
Основным и наиболее частым показанием к операциям на сосудах является кровотечение.
Различают следующие виды кровотечений:
1) по источнику – артериальное, венозное, артериально-венозное и капиллярное (паренхиматозное);
2) по направлению вытекания крови – наружное и внутреннее;
3) по времени возникновения – первичное и вторичное.
Артериальное кровотечение составляет подавляющее большинство кровотечений. По данным ВОВ (1941-1945 г.г.) более 80% всех кровотечений было связано с повреждением артериальных стволов.
Повреждение магистральных артерий представляет две опасности для пострадавших.
1) угрозу смертельного исхода в связи с кровотечением;
2) возможность омертвения дистальной части конечности за счет недостаточности ее питания коллатеральными артериями.
Магистральные артерии разделяются на «безопасные» для перевязки (a.ulnaris, a.radialis, a.tibialis anterior et posterior) – и «опасные» для перевязки (a.subclavia, a.axillaris, a.brachialis, a.femoralis, a.poplitea, a.carotis communis et interna). На данных артериях предпочтительнее производить наложение сосудистого шва или сосудистую пластику. Степень развития гангрены в случаях перевязки магистральных артерий варьирует в очень широких пределах, в зависимости от уровня перевязки артерий и анатомических условий для развития коллатерального кровоснабжения.
При перевязке «опасных» артерий накладывают две лигатуры и между ними пересекают сосуд для десимпатизации нервов адвентиции, расширения коллатералей и улучшения коллатерального кровоснабжения.
Для выравнивания кровяного баланса В.А. Оппель предложил одновременно перевязывать одноименную вену.
Для остановки кровотечения из опасного для перевязки сосуда, хирург должен стремиться к восстановлению непрерывности поврежденного сосуда с помощью сосудистого шва. Если сосудистый шов нельзя выполнить сразу, на относительно короткий промежуток времени можно произвести метод временного протезирования до 72 часов с помощью трубки из синтетических материалов (полихлорвинил, силикон). Промытую (раствором гепарина) трубку вводят в дистальный и проксимальные концы и закрепляют ее лигатурами.
Подход к кровеносному сосуду обычно осуществляется послойным разрезом тканей по проекционным линиям, соответствующим его проекции на кожу.
Если разрез производят строго по проекционной линии, такой доступ называется прямым. Если разрез для обнажения магистрального сосуда производится несколько в стороне от проекционной линии, то такой разрез называют окольным. Например, при обнажении плечевой артерии в средней трети нужно помнить о срединном нерве, находящемся спереди от артерии. Окольный доступ к плечевой артерии осуществляется через влагалище двуглавой мышцы плеча, предотвращающей в последующем вовлечение срединного нерва в послеоперационный рубец.
Показаниями к обнажению и перевязке артерии на протяжении служат:
1) невозможность перевязки сосуда в ране при сильном размозжении тканей, когда эрозированный сосуд находится в толще воспалительного инфильтрата;
2) травматические аневризмы;
3) ампутация конечности при самопроизвольной гангрене, анаэробной инфекции, когда наложение жгута противопоказано.
Перевязка на протяжении по сравнению с перевязкой сосуда в ране применяется значительно реже из-за возможности развития гангрены в ближайшем периоде после операции; возникновения в отдаленные сроки при сохранении жизнеспособности конечности, так называемой «болезни перевязанного сосуда», которая проявляется быстрой утомляемостью конечности, периодически возникающими болями, атрофией мышц из-за относительной недостаточности кровоснабжения тканей.
Перевязку сосудов производят в ране и на протяжении, то есть на некотором расстоянии от места повреждения сосуда.
Сосудистый шов.
Основное показание к наложению сосудистого шва восстановление проходимости магистральных артерий. Различают ручной сосудистый и механический сосудистый швы.
Ручной сосудистый шов бывает боковой и циркулярный. Механический сосудистый шов накладывается при помощи сосудосшивающих аппаратов.
Требования к наложению сосудистого шва.
1. Герметичность. Достигается удалением адвентициальной оболочки сосуда на 2-3 мм от конца, плотным соприкосновением интимы, наложением частого (через 1 мм) непрерывного обвивного шва.
2. Профилактика тромбообразования. Достигается применением антикоагулянтов. Сосудистый шов не должен нарушать ток крови (отсутствие сужения и завихрения); в просвете сосуда должно находиться как можно меньше шовного материала.
3. Профилактика сужения просвета сосуда. Достигается наложением швов-держалок, за которые стенка сосуда растягивается, а непрерывный сосудистый шов не дает стенке сосуда сокращаться до прежних размеров.
Сосудистый шов накладывают вручную с помощью атравматических игл. Механический сосудистый шов достаточно совершенен и не суживает просвета сосуда, но использовать его можно только при плановых операциях и при диаметре сосуда более 2,5 мм.
Сосудистый шов по Каррелю.
1. Доступ к сосуду. Для доступа к сосуду используют проекционную линию по ней или отступя на 1-2 см. Доступ включает послойное рассечение тканей: кожи, подкожной жировой клетчатки, поверхностной фасции, собственной фасции (образующий фасциальный футляр).
2. Мобилизация. Это выделение сосуда из фасциального ложа и сопровождающих его сосудов и нервов. Этот этап включает также наложение сосудистых зажимов Гепфнера отступя от концов сосуда на 1-2 см.
3. Наложение сосудистого шва. Производят иссечение концов поврежденного сосуда, удаление адвентициальной оболочки на 2-3 мм. По Каррелю концы сосуда фиксируют наложением 3 швов-держалок. Используя одну из нитей швов-держалок сосуд между фиксационными швами прошивают непрерывным обвивным швом через 1 мм.
4. Послойное ушивание раны.
Сосудистая пластика.
При наличии большого дефекта применяют трансплантаты из биологического материала. Чаще всего используют аутовену (v. saphena magna, v. basilica).
В качестве трансплантатов в хирургии сосуда используют ауто- и аллотрансплантаты артерий или вен, широко применяют изотрансплантаты из синтетических материалов. Реконструкция производится наложением анастомозов конец в конец или вшиванием трансплантата.
Стентирование.
Стентирование — медицинское оперативное вмешательство, проводимое с целью установки стента — специального каркаса, который помещается в просвет сосудов, например, коронарных сосудов сердца, и обеспечивает расширение участка, суженного патологическим процессом. Стент — это тонкая металлическая трубочка, состоящая из проволочных ячеек, раздуваемая специальным баллоном. Он вводится в пораженный сосуд и, расширяясь, вжимается в стенки сосуда, увеличивая его просвет. Так улучшается кровоснабжение сердца.
LECTURE 7
OPERATIONS ON NERVES
Neororrhaphy, neurolysis (allocation of nerves from the cicatrical tissue) and plasty refer to regenerative operations on peripheral nerves of extremities. The basic indication of these operations is damage. Soft tissues, blood vessels are injured usually during damaging of nerves, there is fracturing of bones.
Nerves of the upper extremities are damaged 1,5 times more often than nerves of the lower extremities.
Damage of nerves is divided into open and closed depending on the condition of the external environment (epineurium). Concussion, injury, compression, dislocation, stretching of nerves refers to closed damages.
Open wounds are accompanied not only by the damage of the epineurium, but also infringement of continuity of axons.
Thus, in injured nerves two processes develop at the same time: degeneration in the peripheral department; and neogenesis in the central department. The central neuroma thickening is formed on the central end of the damaged nerve as a result of inexpedient neogenesis if during neogenesis axons cannot find appropriate empty Shwann’s environments of the distal part of the nerve.
The rate of axon growth in the central part of a nerve into the peripheral end is 1-1,5 mm in a day.
Demands of a neurorrhaphy:
1. Exact compression of nervous fibres fascicles;
2. Nonprojective access (access at 1-2 cm from the nerve projective line);
3. Distance between the ends of the nerve (diastases) up to 1 mm;
4. Suture should pass only if the epineurium is captured
NEURORRHAPHY
It is a nerve stitching operation. Indications are a complete break of a nervous trunk and absence of muscle contraction during examination of electro excitability in a place above a cicatrix. There are primary and delayed neurorrhaphy (early and late). Primary neurorrhaphy is made at the same time with a primary surgical treatment of a wound.
STAGES OF THE OPERATION
- Access. Consists of level-by-level dissection of tissues. Usually access is carried out at a distance of 1-2 cm from the projective line of a nerve.
- Mobilization. Consists of allocation of a nerve from vessels, nerves, muscles near it. This stage of the operation can be called neurolysis if the nerve is involved in the cicatrical tissue.
- Neurorrhaphy. The ends of a damaged nerve excise till there is bleeding from the nerve vessel. Nerve ends are matched to the exact. 3-4 epineuria sutures are imposed. Sutures are tightened till there is easy contact of ends or until there is a distance of up to 1 mm between ends.
- Level-by-level wound suturing and immobilization of the extremity for 2-3 weeks.
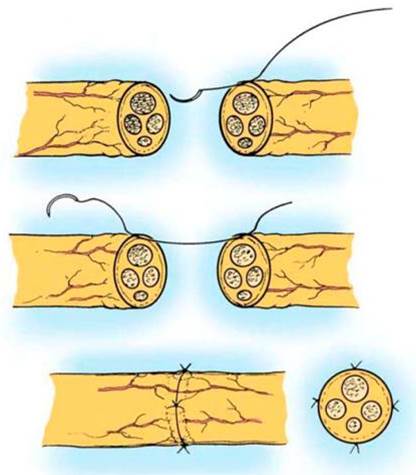
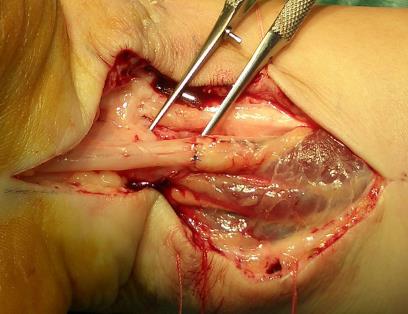
Fig. 17. Transepineurium of the nerves sutures.
NEUROLYSIS
Neurolysis is an operation of mobilization from cicatrical tissues. This operation is carried out better by using an operative microscope. Neurorrhaphy is made during damage of a nerve.
There are internal and external neurolysis.
External neurolysis – is mobilization of a nerve from the cicatrical tissue, placing it over a nerve trunk and causing its compression to be crushed and connected with its functional disorders.
Internal neurolysis – is excision of scars that penetrate into the trunk between its fascicles.
OF PERIPHERAL NERVES
Surgical treatment of nervous trunk injury is difficult during big defects. Nerve diastases of up to 4 cm are liquidated by suturing nerve pieces together without application of additional complex actions. Replacement of nerve defects of 12-20 cm without using special receptions is impossible. Two methods are applied here: rapprochement of nerve ends and plastic replacement.
1. Rapprochement of nerve ends is reached by mobilization of the nervous trunk to a long extent and changing of extremity position (flexion – extension in a joint or in combination with extension of nerves).
2. Rapprochement of nerve ends may be carried out by changing the topography-anatomic position of the nerve (during big diastases). This allows the nerve suturing of defects of 10-11 cm.
3. Rapprochement of nerve ends is reached with the help of bone resection if bone trauma and nerve defect have occurred at the same time (on upper extremity).
OPERATIONS ON TENDONS
Damage of tendons leads to functional disorders of extremities which are eliminated only by surgical operations.
The most common type of operation on tendons is tendon suturing.
Suturing of a tendon, J.J. Dzhanelidze, especially during operations of the hand and forearm are carried out as follows:
1. To grasp the minimal amount of tendon fascicles.
2. To provide a smooth, slippery surface on the tendon.
3. Don't suppose garneting of tendon.
4. Don't compress the vessels supplying the tendon.
Primary and secondary sutures of tendons are distinguished in dependence on the operation time after trauma. Initial suturing is made – during the first 6-8 hours after trauma on clean surfaces and a small zone of soft tissues that are damaged.
Secondary suture is imposed after wound repair with first intentions of within 2-3 weeks. If the wounds were purulent, the operation is postponed to the 3-4th months.
Tendons sutures are classified into 4 groups according to the location of the strings and knots.
1. Strings and knots outside (on the tendon surface).
2. Strings inside, knots outside.
3. Strings and knots inside.
4. Other.
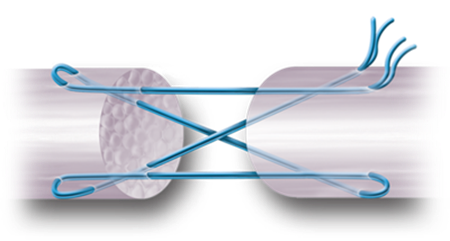
Fig. 18. Strings inside, knots outside.
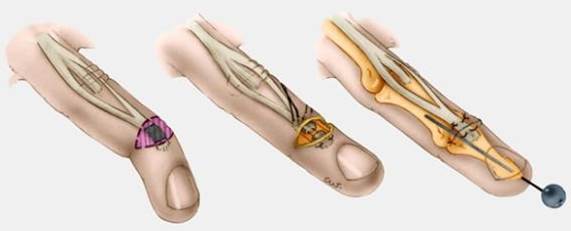
Fig. 19. Other group.
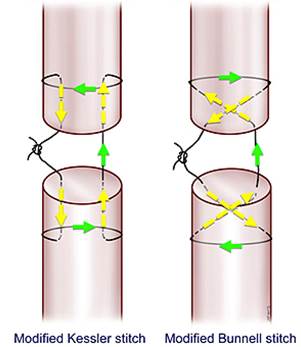
Fig. 20. Strings and knots inside
STAGES OF THE OPERATION
1. Access. Extra projective access is usually at 1-2 cm from the tendon projective line.
2. Mobilization or tenolysis which involves a tendon in cicatrical tissue.
3. Tenosuture. The ends of the damaged tendon are excised. Special tendon suture is imposed.
4. Level-by-level suturing of wounds and immobilization of extremity.
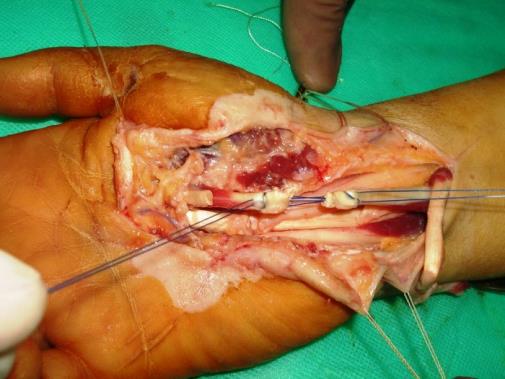
Fig. 21. Operations on tendons
PLASTIC OPERATIONS
Plastic operations are the most common types of operations on tendons which consist of elongation or shortening of tendons, transplantations and moving of a tendon.
Elongation or shortening of tendons without infringement of its continuity is made with the purpose of improvement of muscle function.
Elongation of tendons is carried out with the help of a Z-shaped dissection of the tendon in the sagittal or frontal plane with the subsequent suturing of tendon ends. Other sections are rarely applied to elongation of tendons, such as slanting, three and four-stage, transversal and their various combinations.
Shortening of tendons is made by its resection on extent or formation of dublication.
TENDON TRANSPLANTATION
Tendon transplantation serves mainly for the correction of unsuccessful tendon sutures and for replacement of large defects. Pieces of tendons taken in the operation are material for autoplastic replacement of tendon defects.
MOVING OF A TENDON
It is applied for replacement of muscles that have lost their function because of neighboring healthy muscles. So tendons of functioning muscles are cut entirely from the place of attachment and moves in a new bed.
Tenotomy – is an operation of tendon section. This operation is made for elimination of the excessive draft of muscles.
Tenolysis – is an operation consisting of tendon mobilization from cicatrical solderings with surrounding tissues.
Tenodesis – is fixation of one or several tendons of paralysed muscles subperiostalis (tenoperiosteodesis) or in specially prepared osteal canal (tenoosteodesis).



Fig. 22. Operations on tendons
|
|
|
ОПЕРАЦИИ НА НЕРВАХ.
На периферических нервах конечностей из восстановительных операций производят шов нерва, невролиз (выделение нерва из рубцовой ткани) и пластику. Основным показанием к этим операциям является повреждение. Обычно при повреждении нервов повреждаются мягкие ткани, кровеносные сосуды, имеются переломы костей.
Нервы верхних конечностей повреждаются в 1,5 раза чаще, чем нервы нижних конечностей.
В зависимости от состояния наружной оболочки (эпиневрия) повреждения нервов делятся на открытые и закрытые. К закрытым повреждениям относятся: сотрясение, ушиб, сдавление, вывих, растяжение нерва.
Открытые ранения сопровождаются не только повреждением эпиневрия, но и нарушением непрерывности аксонов.
При этом, в поврежденном нерве одномоментно развиваются два процесса: в периферическом отделе – дегенерация; и в центральном отделе – регенерация. Если в процессе регенерации аксоны «не найдут» соответствующих пустых швановских оболочек дистального отрезка нерва, то в результате нецелесообразной регенерации на центральном конце поврежденного нерва образуется утолщение – центральная неврома.
Скорость прорастания аксонов центрального отрезка нерва в периферический конец соответствует 1-1,5 мм в сутки.
Требования к шву нерва:
1. Точное сопоставление пучков нервных волокон;
2. Внепроекционный доступ (доступ, отступя от проекционной линии
нерва на 1-2 см);
3. Расстояние между концами нерва (диастаз) до 1 мм;
4. Шов должен проходить только с захватом эпиневрия.
НЕВРОРАФИЯ.
Операция наложения шва нерва. Показаниями служат полный перерыв нервного ствола, а также отсутствие сокращения мышц при исследовании электровозбудимости выше рубца. Различают первичный и отсроченный шов нерва (ранний и поздний). Первичная нейрорафия производится одновременно с первичной хирургической обработкой раны.
Этапы операции:
1. Доступ. Заключается в послойном рассечении тканей. Обычно доступ проводят отступая от проекционной линии нерва на 1-2 см.
2. Мобилизация. Заключается в выделении нерва от расположенных рядом сосудов, нервов, мышц. При операции на нервах этап может называться невролиз, если нерв вовлечен в рубцовую ткань.
3. Неврорафия. Шов нерва. Иссекают концы поврежденного нерва до появления кровотечения из сосудов нерва. Точно сопоставляют концы нерва. Накладывают 3-4 эпиневральных шва. Швы затягивают до легкого соприкосновения концов или до расстояния между концами до 1 мм.
4. Послойное ушивание раны и иммобилизация конечности на 2-3 недели.
НЕВРОЛИЗ.
Невролиз это операция по освобождению нервного ствола из рубцовой ткани. Эту операцию лучше всего выполнять с использованием операционного микроскопа. При повреждении нерва производят шов нерва.
Выделяют внутренний и внешний невролиз.
Внешний невролиз - это освобождение нерва от рубцовой ткани, располагающейся снаружи нервного ствола и вызывающей его сдавление, ущемление и связанные с этим функциональные расстройства.
Внутренний невролиз - это иссечение рубцов, проникающих внутрь ствола между его пучками.
Этапы операции.
1. Доступ. Чаще делают внепроекционный доступ, на 1-2 см от проекционной линии сухожилия.
2. Мобилизация или тенолиз при вовлечении сухожилия в рубцовую ткань.
3. Тенорафия. Концы поврежденного сухожилия иссекаются. Накладывается специальный сухожильный шов.
4. Послойное ушивание раны и иммобилизация конечности.
Пластические операции.
Частым видом оперативных вмешательств на сухожилиях являются пластические операции, которые заключаются в удлинении или укорочении сухожилия, пересадки и перемещении сухожилия.
Удлинение или укорочение сухожилия без нарушения его непрерывности производится с целью улучшения функции мышц.
Удлинение сухожилия осуществляется с помощью Z-образного рассечения сухожилия в сагиттальной или фронтальной плоскости с последующим сшиванием концов сухожилия. Реже для удлинения сухожилия применяются другие разрезы - косые, трех- и четырехступенчатые, поперечные и их различные сочетания.
Укорочение сухожилия производится путем его резекции на протяжении или образование дубликатуры.
Пересадка сухожилия.
Пересадка сухожилия служит главным образом для коррекции безуспешных сухожильных швов и для замещения крупных дефектов. Материалом для аутопластического замещения дефекта сухожилия служат отрезки сухожилий, взятых в области операции.
Перемещение сухожилия.
Применяется для замещения утраченной функции одних мышц за счет здоровых соседних мышц. При этом сухожилия функционирующей мышцы отсекается целиком от своего места прикрепления и перемещается в новое ложе.
Тенотомия - операция рассечения сухожилия. Это оперативное вмешательство производится для устранения чрезмерной тяги мышц.
Тенолиз - оперативное вмешательство, заключающееся в освобождении сухожилия от рубцовых спаек с окружающими тканями.
Тенодез - фиксация одного или нескольких сухожилий парализованных мышц поднадкостнично (тенопериостеодез) или в специально подготовленном костном канале (теноостеодез).
LECTURE 8
PUNTURE OF JOINTS
Puncture of joints are performed in order to see the state of the contents of the joint cavity (blood, pus), to remove the pathological fluid, to apply antibiotics.
To anasthetize the zone of puncture, 0, 5% Novocaine solution is injected with a fine needle. Before the punture of the joint the tools are prepared, the surgeon’s arms and the operation room is treated like in most common types of operations. It is necessary to remember that joints are susceptible to infections as the articular fluid can serve as a medium for growth of microflora, therefore the inflammation of joint is often associated with septic effects.
Skin on the place of puncture is shifted aside to get the curve of the wound canal when the skin returns to its place after the puncture. A thick needle (sometimes even a thin trocar) is introduced into the joint cavity. When the needle reach the joint the resistance noted during passage of the needle through soft tissues diminishes. After the removal of the needle the place of puncture is covered with collodium or plaster.
Puncture of the elbow joint
A forearm is bent to make a right angle. The needle is then injected from outside between the external condyle of the humerus bone and the ulnar process and run to the joint cavity above the head of the radial bone. To perform the puncture of the upper volvulus of the joint the needle is introduced above the olecranon apex and run downward and forward.
Fig 27. Humeral Arthrocentesis
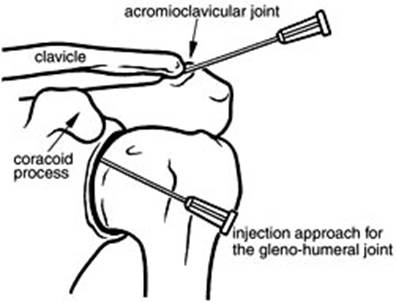
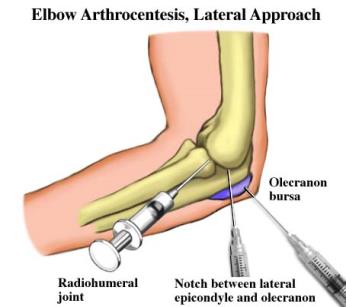
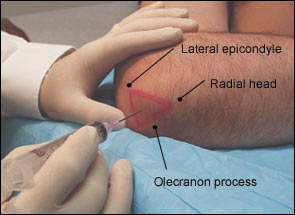
Fig 28. Puncture of elbow.
Puncture of the radiocarpal joint is performed on the dorsal surface of the hand. The projection of the joint corresponds to the line connecting the styloid process of the ulnar and the radial bones. The joint is punctured in the cross point of the connecting lines being the the continuation of the second metacarpal bone. The needle hits the joint between the long extensor tendons of the thumb and the extensor of the second finger.
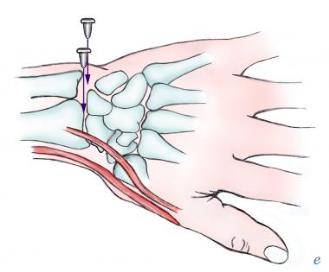
Fig 29. Puncture of a metacarpal joint.
Puncture of a hip joint
A needle is run in the frontal plane inside above the apex greater trochanter of the hip to cavity of acetabulum. The puncture can be performed from the front surface of the hip. The greater trochanter and the middle of poupart ligament are connected with a line its middle point corresponding to to the femoral head. The needle is introduced in this point at right angle to the skin and ran deep inside.
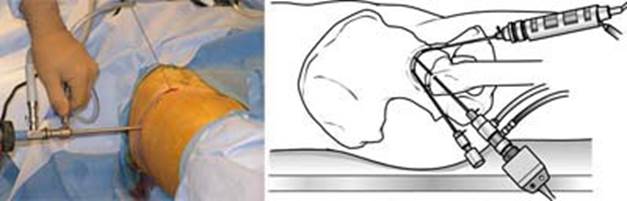
Fig 30. Puncture of a hip joint.
Puncture of the knee joint
The needle is introduced from the outer or inner side of the patella at the level of its middle height reaching between its back surface and front surface of the lower metaphysis of the hip. The top volvulus is punctured running the needle under the top point of the patella.
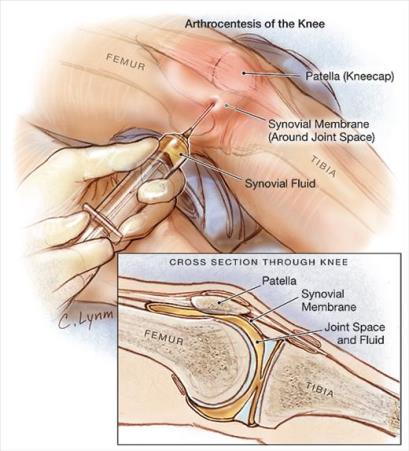
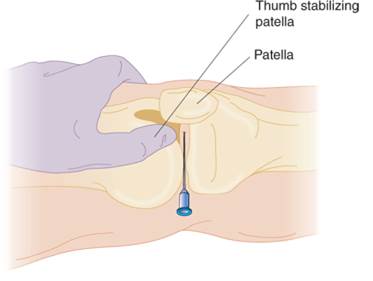
Fig 31. Puncture of the knee joint
Puncture of the ankle joint
The needle is injected 1, 5-2cm above and inward from the lateral malleolus apex. The needle is run backward horizontally with some down inclination and medially between lateral malleolus and long extensor tendon of the fingers. The joint cavity can be reached from the medial side. The needle is injected 1 cm higher than medial malleolus apex. The needle is than ran between the medial malleolus and anterior tibial muscle tendon.

Fig 32. Puncture of the ankle joint
RESECTION OF JOINTS
The indication for arthrectomy is gun shots wounds of articular ends, tuberculosis of joints, and purulent arthritis with epiphysises involvement.
The operation includes partial or complete removal of bone ends together with cartilages and the synovial membrane. After complete resection the adhesion of the osteal ends and the stiffness of the joint follow (ankylosis). In these cases the plane bone saw is used for resection. Bone saw-lines are brought together and fixed in the best position for reserve the extremity function. The resection may be performed without the opening of the articular cavity (extra-articular resection).
Knee replacement.
Knee replacement, also known as knee arthroplasty, is a surgical procedure to replace the weight-bearing surfaces of the knee joint to relieve pain and disability. It is most commonly performed for osteoarthritis,[1] and also for other knee diseases such as rheumatoid arthritis and psoriatic arthritis. In patients with severe deformity from advanced rheumatoid arthritis, trauma, or long-standing osteoarthritis, the surgery may be more complicated and carry higher risk. Osteoporosis does not typically cause knee pain, deformity, or inflammation and is not a reason to perform knee replacement.
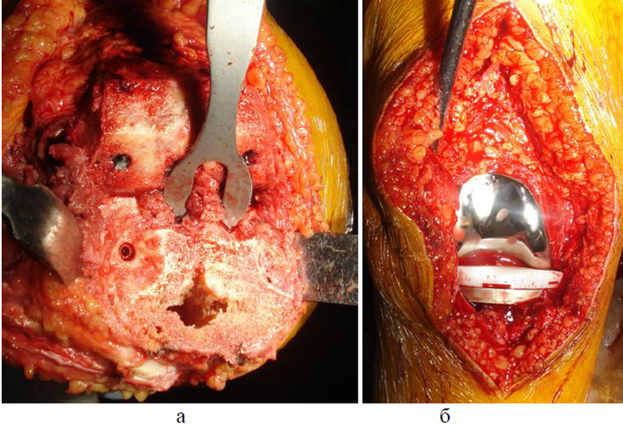
Fig 34. Knee replacement.
Тема 8.
ПРОКОЛ (ПУНКЦИЯ) СУСТАВОВ.
Прокол сустава производят с целью выяснения характера содержимого полости сустава (гной, кровь), для эвакуации патологической жидкости, для введения антибиотиков.
С целью обезболивания зоны прокола применяют 0,5% раствор новокаина, который вводят с помощью тонкой иглы. Перед проколом сустава проводят подготовку инструментария, рук хирурга и операционного поля, как при проведении всякого хирургического вмешательства. Необходимо помнить о том, что суставы восприимчивы к инфекции, так как суставная жидкость является как бы питательной средой для развития микрофлоры, поэтому воспаление суставов часто протекает с септическими явлениями.
Кожу в месте прокола сдвигают в сторону, чем достигается искривление раневого канала при возвращении кожи на свое место после окончания пункции. На шприц надевают толстую иглу (иногда пользуются даже тонким троакаром) и вводят ее в полость сустава. В момент попадания иглы в сустав исчезает сопротивление, которое отмечалось во время прохождения через мягкие ткани. После извлечения иглы место прокола следует заклеить коллодием или пластырем.
Прокол плечевого сустава. Спереди иглу вводят под клювовидный отросток лопатки и продвигают кзади между ним и головкой плечевой кости на глубину 3—5 см. Снаружи можно попасть в сустав, проводя иглу между плечевым отростком лопатки и головкой плечевой кости снаружи внутрь и книзу. Сзади иглу вкалывают в ямку, образованную плечевым отростком лопатки и задним краем дельтовидной мышцы, проводят ее снизу вверх и кпереди, нацеливая на клювовидный отросток, на глубину 4—5 см.
Прокол локтевого сустава. Предплечье сгибают в локтевом суставе под прямым углом. Иглу вкалывают снаружи между наружным мыщелком плеча и локтевым отростком и продвигают в полость сустава над головкой лучевой кости. Для пункции верхнего заворота сустава прокол иглой делают над верхушкой оleсгаnon и следуют вниз и кпереди.
Прокол лучезапястного сустава делают на тыле кисти. Проекция сустава соответствует линии, соединяющей шиловидные отростки локтевой и лучевой костей. Пунктируют сустав в точке пересечения указанной линии с линией, являющейся продолжением второй метакарпальной кости. Игла проникает в сустав между сухожилиями длинного разгибателя большого пальца и собственного разгибателя II пальца.
Прокол тазобедренного сустава. Иглу продвигают во фронтальной плоскости снаружи внутрь над верхушкой большого вертела бедра по направлению к вертлужной впадине. Можно произвести пункцию и с передней поверхности бедра. Большой вертел и середину пупартовой связки соединяют линией, середина которой соответствует головке бедренной кости. Иглу вкалывают в этой точке под прямым углом к коже и направляют затем вглубь и кнутри.
Прокол коленного сустава. Иглу вводят с наружной или внутренней стороны надколенника на уровне середины его высоты, проникая между его задней поверхностью и передней поверхностью нижнего метафиза бедра. Верхний заворот пунктируют, проводя иглу под верхний полюс надколенника.
Прокол голеностопного сустава. Иглу вкалывают на 1,5—2 см выше и кнутри от верхушки наружной лодыжки. Иглу при горизонтальном положении с некоторым наклоном вниз проводят спереди назад и медиально между наружной лодыжкой и сухожилием общего длинного разгибателя пальцев. Попасть в полость сустава можно и с медиальной стороны. Для этого иглу вкалывают на 1 ем выше верхушки внутренней лодыжки. Игла проходит между внутренней лодыжкой и сухожилием передней большеберцовой мышцы.
ВЫЧЛЕНЕНИЕ (ЭКЗАРТИКУЛЯЦИЯ) ПАЛЬЦЕВ КИСТИ.
Экзартикуляцией называют удаление дистальной фаланги пальца на уровне сустава. Операция осуществляется с образованием лоскутов, которыми укрывают головки пястных костей. Кожные лоскуты выкраивают с таким расчетом, чтобы рубцы не располагались на рабочей поверхности. Для I, III и IV пальцев рабочей поверхностью является ладонная, для II пальца — лучевая и ладонная, для V пальца — локтевая и ладонная.
Удаление III и IV пальцев делают разрезом по Люппи. Проводят круговой разрез до кости на уровне ладонно-пальцевой складки.. На тыльной поверхности основной фаланги производят дополнительный срединный продольный разрез, который начинают от головки пястной кости и соединяют с круговым. Образовавшиеся лоскуты отсепаровывают в стороны. Проникают-скальпелем в пястно-фалангеальный сустав и, рассекая суставную капсулу с боковыми связками, удаляют палец. Перевязывают пальцевые артерии. Можно сшивать над головкой пястной кости сухожилия сгибателей и разгибателей.
Удаление II и V пальцев делают разрезом по Фарабефу. На II пальце разрез ведут по тыльной поверхности от линии пястно-фалангового сустава дугообразно к середине длины лучевой поверхности основной фаланги. Отсюда разрез направляют через ладонную поверхность основной фаланги к локтевому краю пальца, не доходя 2 мм до межпальцевой складки. Начальную и конечную точки разреза соединяют дополнительным разрезом. Образованный ладонно-лучевой кожный лоскут отделяют. Удаляют палец, пересекая скальпелем боковые связки и капсулу сустава. Перевязывают пальцевые артерии. Выкроенный лоскут пришивают шелковыми швами к оставленной кромке кожи на локтевой поверхности удаленного пальца. При удалении V пальца выкраивают лоскут на ладонно-локтевой поверхности основной фаланги мизинца.
Удаление большого пальца делают разрезом по Мальгеню. Разрез на ладонной стороне пальца проводят на 0,5 см проксимальнее межфаланговой складки, а на тыле пальца следуют на 0,3 см дистальнее пястно-фалангового сустава. После рассечения мягких тканей по линии эллипса образовавшийся на ладонной поверхности лоскут кожи отсепаровывают. Удаляют палец теми же приемами, стараясь сохранить переднюю стенку суставной сумки с сесамовидными косточками, к которым прикрепляются мышцы, способные в дальнейшем управлять движениями оставшейся метакарпальной кости. После перевязки сосудов накладывают швы на кожную рану.
РЕЗЕКЦИЯ СУСТАВОВ
Показанием к резекции сустава является огнестрельные ранения суставных концов, туберкулез сустава, гнойный артрит с поражением эпифизов.
Оперативное вмешательство предусматривает частичное или полное удаление суставных концов костей вместе с хрящами и синовиальной оболочкой. После полной резекции наступает сращение костных концов и возникает неподвижность сустава (анкилоз). В этих случаях в месте резекции выполняют плоскостной опил костей. Опилы костей сводят друг с другом и закрепляют в выгодном для функции конечности положении. Резекция может проводиться без вскрытия его полости – внесуставная резекция.
РЕЗЕКЦИЯ КОЛЕННОГО СУСТАВА (ПО МЕТОДУ ТЕКСТОРА).
Дугообразным разрезом мягких тканей, выпуклостью обращенной вниз, при согнутом колене соединяют задние края обоих мыщелков бедра. На голени линия разреза проходит на 1-2 см. ниже бугристости большеберцовой кости. Выделив передний лоскут вместе с надколенником, вскрывают полость сустава, пересекают его боковые и крестообразные связки, обнажают мыщелки бедра. Спиливают полностью суставные поверхности надколенника, бедра и большеберцовой кости. Удалив сумку сустава, концы костей сближают и фиксируют кетгутовыми швами. Концы пересеченной собственной связки надколенника сшивают. Накладывают швы на кожу. Конечность фиксируют под углом 170-175 градусов гипсовой повязкой, для формирования анкилоза в функционально выгодном положении.
LECTURE 9
Amputations.
Amputation of an extremity dissecting along the length of the bone. The indications for amputation are non-vital extremity (complete abruption of an extremity, extensive crushing damage of tissues, damage of vessels and nerves), progressing infection (mainly anaerobic), gangrene of an extremity, burns, frost bites etc. Reamputations are performed in defects of an amputated stump, interfering its function and prosthetic treatment.
The degree of amputation is done according to line of vital tissues and by the degree of the destruction of the bone. The amputation of upper extremities should be performed in best economic way. Amputations are performed using tourniquet, except for amputations in patients with atherosclerosis or oblitering endarteritis.
When making an incision bear in mind of the future prosthetic treatment. The end of the stump shouldn't have scar. To prevent defective stump, the muscles are dissected 4-5cm distally from the bone being cut since muscles contract after dissection. Arteries and veins are lighted, large arteries are sutured. Hemostasis is done carefully. Nerves are cut using a razor 4-5cm above the end of the stump. The soft tissues are sutured in layers forming the scar mobile and away from the place of future contact with prosthesis. For the upper extremity such place is the palmar surface, for the lower extremity- the front surface of a stump. Depending on the type of incision on soft tissues the amputations are divided into: circular (guillotine, one staged, two staged, three staged), flapped (one flapped, two-flapped) and osteoplastic.
Guillotine amputation
All soft tissues and bones are dissected on the same level. Such amputations are performed quickly, enabling the control of infections especially anaerobic, allows saving the maximum length of an extremity. A disadvantage of operation is formation of defective stump due to contraction of soft tissues and exposure of the bone, the process of healing takes a long, terminal osteomyelitis may develop. Therefore this amputation is performed seldom to prevent the development of an infection.
One--staged amputation
One-staged amputation involves circular dissection of skin, subcutaneous fat and fascia and subsequent dissection of muscles and bone above the incision.
Reamputation is always indicated after one-staged amputation to form full functioning stump.
Two-staged amputation
The skin, subcutaneous fat and fascia are dissected, then the muscles are dissected at the level of the skin, drawn off in a proximal direction and the bone is sawn at the level of where muscles were drawn off. Another technique of this operation is the amputation of the forearm in its lower third using the cuff. The circular dissected skin, subcutaneous fat and fascia are separated simultaneously in a cuff and turned back in proximal direction.
Flapped amputation
For this kind amputation one or two flaps maybe performed. For one-flapped method the length of the skin flap should be equal to the diameter of an extremity on the level of amputation that is 1/3 of the circle. For two-flapped method one of the flaps is made longer than the other. Their total length should be equal to the diameter. It is necessary to add several cm to allow skin contraction. Skin contraction on the flexor surface of an extremity is more on the extensor surface. The flap may consist of skin with subcutaneous fat (dermal flap) or may include skin with muscles (myosplastic flap), skin with tendons (tendoplastic flap), and skin with muscles, periosteum and bone (osteoplastic).
The technique of any amputation includes four stages:
1 stage - of soft tissue dissection. To one of the methods mentioned before
2 stage - dissection of periosteum and bone sawing
a) Periosteal-on the periosteum level
b) Aperiosteal- 2-5mm below periosteal level (in osteoplastic operations)
c) Subperiosteal-sawing the bone with subsequent closing of bone-saw line with periosteum ( in children)
3 stage- ligation of all the vessels and truncation of nerves 4-5cm above the level of amputation
4 stage- formation of stump acc to of the methods mention

Fig 36. Flapped amputation
AMPUTATION OF THE HIP
Amputation of the hip is done at its middle third to Pirogov cone-circular three-staged method. Vessels are isolated and ligated, nerves are truncated. Skin is sutured with silk. Drainage tubes are inserted into the angles of the wound. The extremity is fixed with plaster splint.
LECTURE 1 0
ANATOMIC TOPOGRAPHY OF HEAD
(CEREBRAL PART)
Cerebral cranium is divided into: calvarium (fornix crani) and basis (basis crani). Calvarium is divided into four areas: fronto-parieto-occipital, temporal, aural and mastoidal.
MASTOIDAL AREA (REGIO MASTOIDEA)
This region corresponds to the processus mastoideus. Skin is thin, and its posterior part is covered with hair. Subcutaneous fatty tissue is less, a. et v. auricularis posterior pass through it. Fascia is thin in upper part and is separated with difficulty towards the apex of the process.
Periosteum is dense, easily separates from the anterior smooth surface of the process; on the posterior part, it is connected with the rough surface of the process at the point of attachment of m. sternocleidomastoideus.
Bone of the process contains cellula mastoidea of different sizes, lined by tunica mucosa. They form one big cellula: antrum mastoideum, which communicates with the cavity of middle ear through aditus ad antrum. Antrum mastoideum lies in anterio-superior square, 2 mm behind from external aditus meatus. It is projected in Shipo triangle. Anterior border of the triangle- line going from spina suprameatus Henle to the apex of processus mastoideus. Posterior border- crista (tuberositas) mastoidea, upper border- horizontal line, as the continuation of zygomatic arch (linea temporalis). N. facialis is projected in front of the triangle; behind the triangle lies S-shaped sinus sigmoideus and higher lies fossa cranialis medialis.
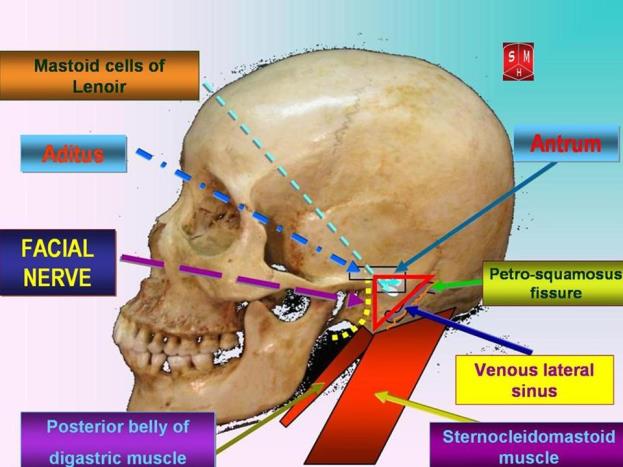
Fig 45. Mastoid area
BLOOD SUPPLY TO BRAIN
Paired arteries: aa. carotis interna et aa. vertebralis supply blood to brain. The two vertebral arteries join at the base of skull to form a. basilaris. Two aa. cerebri posterioris branch out from a. basilaris, while from a. carotis interna- a. cerebri media, a. cerebri anterior and a. communicans anterior. Hence forms circulus anteriosus cerebri (Wilisii) which lies in the subarachnoid space at the base of the brain and surrounds sella turcica and chiasm of optical nerves.
Cronlein’s scheme, further added by S.S. Brjusova is recommended for the projection of sulcus, gyrus of brain and vessels on the surface of calvarium. Following lines are applied on the skin of the head:
1) lower horizontal- follows through the lower margin of orbit.
2) upper horizontal- goes parallel to first one through superior margin of orbit.
3) median line- follows suture sagittalis.
4) anterior- vertical- passes through the mid of zygomatic arch.
5) medial-vertical- passes through the middle of processus condylaris of mandibula
6) posterior-vertical- through base of processus mastoideus.
7) line connecting the crossway of 2nd and 4th lines with 6th line.
8) line representing the bisector angle, formed by the 7th line and the 2nd line.
9) Brjusov’s line- passes parallel to 2nd line through the crossing point of 6th and 8th line.
Central (Roland’s) sulcus corresponds to the scheme of 7th line, occupying from second and third verticals. Anterior central gyrus of brain lies in front of this line while posterior central gyrus of brain lies behind it. Projection of Sylvian’s sulcus corresponds to the scheme of 8th line.
The main trunk of a. meningea media is projected on the crossing point of first vertical and upper margin of zygomatic arch. Anterior branch passes through the crossing point of first vertical with 2nd line, posterior branch- through the crossing point of posterior vertical with the same 2nd line.
Location of internal carotid artery along the sinus cavernosus is projected on the anterio-inferior quadrangual scheme (Bergman quadrangle). Otogenic abscesses are also located here.
A. cerebralis anterior corresponds to horizontal Brjusov’s line. The place of division of a. cerebralis medialis corresponds to the crossing point of 2nd and 4th line. A. cerebralis posterior is projected above medial horizontal line in its posterior part.
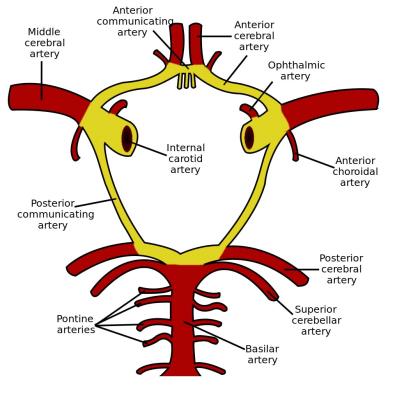
Fig 47. Blood brain to supply.
Fig 48. Krenlein scheme.
ТЕМА 10.
LECTURE 11
REGIO ORBITALIS
There are two sections in orbit: superficial- region palpebralis and deep- region orbitalis propia, where the eyeball with muscles, vessels, nerves and fatty tissue (corpus adiposum orbitae) are located.
Regio orbitalis propria has 4 walls:
1) paries superior- formed by os. frontalis et os sphenoidale alae minor. Fossa gl. lacrimalis is present here.
2) paries inferior- formed by orbitalis maxillae. Here lies sulcus et canalis infraorbitalis.
3) paries lateralis- formed by os. zygomaticus et os sphenoidale alae major. Here lies for. zygomaticoorbitale.
4) paries medials- formed by lam. orbitalis ossis ethmoidalis et os lacrmale. Here lies foramen ethmoidale anterius et posterius et canalis nasolacrimalis.
On the border of paries superior et paries lateralis, fissure orbialis superior is located, through which vessels and nerves pass:
1) n. oculumotorius- innervates mm. rectus inferior, medialis, superior et m. levator palpebrae superior et m. obliqus inferior and takes part in the formation of gangl. ciliare;
2) n. trochlearis- innervates m. obliqus superior;
3) n. abducens- innervates m. rectus lateralis;
4) n. opthalmicus- forms:
-n. frontalis, which divides into two branches: n. supratrochlearis- innervates skin of upper eyelid, and n. supraborbitalis- innervates skin of forehead;
-n. larcimalis, which innervates gl. lacrimalis;
-n. nasociliaris, which divides into: nn. ethmoidalis anterior et posterior- innervates nasal cavity, n. infratrochlearis- innervates skin of lower eyelid, r. communicans cum ganglio ciliary;
5) v. opthalmica superior- opens in sinus cavernosus.
On the border of paries inferior et paries lateralis, fissure orbitalis is located which connects region orbitalis with fossae pterygopaltina et infratemporalis. Through it pass: a. et n. infraorbitalis, n. zygomaticus, v. infraorbitalis.
Canalis opticus is present on the apex of orbital pyramid, through which pass: n. opticus- innervates retina of eye; a. opthalmica- from which branch out: aa. ethmoidales anterior et posterior, a. supraorbitalis, supratrochlearis, and also other branches – bulbus oculi, m. opthalmicus, gl. lacrimalis. A. opthalmica forms anastomosis with a. dorsalis nasi.
Bulbus oculi consists of three layers:
1) external- tunica fibrosa bulbi- divides into two parts: sclera and cornea.
2) middle- tunica vasculosa bulbi- divides into: a) iris (at the centre of which lies pupil along with m. dilator pupillae, m. sphincter pupillae), ciliary body (corpus ciliare) - lies around lens and c) vascular membrane (choroidea).
3) internal- retina, with spot of retina (macula) that lies in fovea centralis, papillae nervi opticus is located inside where visual sensation is absent- blind spot (macula coeca).
Camera anterior et posterior bulbi lie in front of the lens. Most part of bulbus oculi is filled by vitreous body (corpus vitreum), having jelly like consistency.
Fig 49. Regio orbitalis propria.
REGIO NASALIS
Borders: upper- glabella, lower- linea horizontalis septum nasi, lateral- sulcus nasobuccalis.
Nasal region comprises of: external nose (nasus externa) - which contains bony and cartilaginous mass; nasal cavity (cavum nasi).
Nasus externa represents: os nasale, processus frontalis maxillae et cartilagines nasi lateralis, cartilagines alares majoris et minors. Blood supply: a. dorsalis nasi (a. opthalmica), a. angularis (a. facialis). Venous blood outflow occurs through v. dorsalis nasi and v. angularis. Innervation of wings and tip of nose- n. ethmoidalis anterior; dorsum of nose- n. infraorbitalis.
Cavum nasi contains 6 walls:
1) anterior- formed by nasus externa et nares;
2) posterior- formed by choanae;
3) superior- represented by lamina cribosa ossis ethmoidalis et corpus ossis sphenoidalis. Apertura sinus sphenoidalis lies here;
4) inferior- represented by palatinum durum et palatinum molle. Here lies canalis incisivus, for. palatinum majus et minor.
5) external- represented by 3 conchae nasalis: superior, media et inferior. Foramen sphenopaltinum, for. ethmoidalia anteriorus et posteriorus are located here.
6) internal- represented by septum nasi.
Fig 50. Region nasalis.
Cavum nasi consists of 3 nasal courses:
- meatus nasi superior: cellulae etmoidales posterioris opens here;
- meatus nasi medius: aperture sinus frontalis, hiatus maxillaries et cellulae ethmoidales anteriores et mediae open here;
- meatus nasi inferior: canalis nasolacrimalis open here.
Blood supply of nasal cavity is performed by branches of a. carotis externa (a. facialis, a. maxillaries- a. sphenopalatina, palatine descendens) et a. opthalmica (a. ethmoidales anterior et posterior, a. dorsalis nasi).
Venous outflow occurs along the veins of the same name into: plexus venous pterygoideus et sinus cavernosus et v. facialis.
Innervation takes place by the following nerves: nn. olfactorius, nn. ethmoidales anterior et posterior; rr. nasalis posterioris et n. nasopalatinum- ganglion pterigopalatinum.
REGIO ORALIS
Regio oralis contains:
1) rima oris- contains: cutis, fascia superficialis, m. orbicularis oris, mm. zygomaticus major et minor, m. levator labi superioris alaeque nasi, m. levator anguli oris, m. depressor anguli oris et inferioris. Here pass- a. et n. labiales superior et inferior, tunica mucosa forms frenicum labi superior et inferior. N. facialis innervates all mimic muscles.
2) cavitas oris consists of: vestibulum oris et cavitas oris propria.
Vestibulum oris- slit-like space bounded by: outside- buccae, labium superior et inferior, rima oris; inside- dentes, gingivae, processus alveolaris maxillae, pars alveolaris mandibulae. It contains two archs: vestibulum oris superior et inferior, here lies frenulum labi superioris et inferioris. On the tunica mucosa of buccae, at the level of 1 or 2 superior molar lies papilla parotidea, where ductus parotideus opens.
Cavitas oris propria- bounded by: anteriorly and laterally- dentes, gingivae; superiorly- palatum; inferiorly- fundus cavitas oris, lingua; posteriorly- fauces connecting with pars oralis pharynges.
Palatum durum consists of: processus palatinus maxillae et lamina horizontalis ossis platini forming raphe palate where canalis incisivus is located. At the level of 8 upper molar lies for. palatina majus et minora.
Palatum molle represents m. tensor veli palatine, m. levator veli palatine, m. uvulae, m. palatoglossus, m. palatopharyngeus. Blood supply is done by- a. palatine descendens(a. maxillaries)- aa. palatine major et minors, a. palatine ascendens et tonsilaris (a. facialis). Venous outflow occurs in plexus pterygoideus et pharyngeus. Innervation takes place by branches of ganglion pterygopalatinum- n. palatinus major et n. nasopalatinus, rr. pharyngei- n. glossopharyngei, n. vagi m. tensor veli palatine is innervated by n. mandibularis. Remaing muscles by plexus pharyngeus.
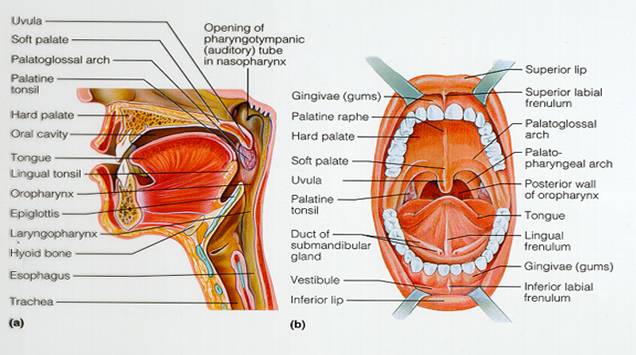
Fig 51. Cavum oris.
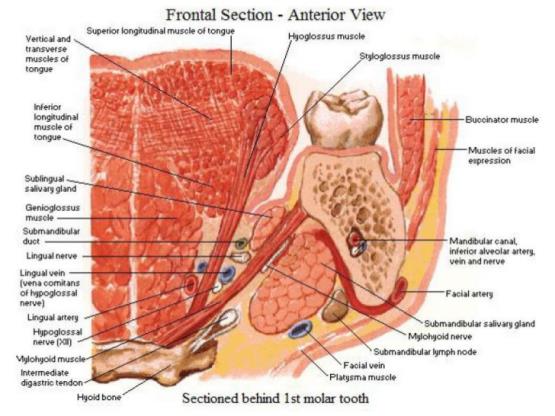
Fig 52. Cavum oris.
Fundus cavitas oris is formed by diaphragm oris- m. mylohyoideus, where- m. geniohyoideus et genioglossus, m. hyoglossus, m. styloglossus, m. palatoglosus- form basis of lingua. The own muscles of lingua are- m. longitudinalis linguae superior et inferior, m. transverses linguae, m. verticalis linguae. Ductus submandibularis along with ductus sublingualis open at the basis of its frenulum. Blood supply of tongue (lingua)- a.v. lingualis, innervation- n. lingualis( n. mandibularis), chorda tympani, n. glossopharyngeus, hypoglossus, n. laryngeus superior (n. vagus).
REGIO BUCCALIS
Borders of regio buccalis: upper- margo inferior os zygomaticus; lower- margo inferior os mandibulae; anterior- sulcus nasolabialis, posterior- m. masseter.
Skin is thin, elastic and contains hair. The subcutaneous fatty tissue contains: m. zygomaticus major, m. risoris, m. depressor anguli oris, m. buccinators, innervated by n. facialis. Below mimic muscles lie, intermuscular cellulose space, in which passes a. facialis (a. carotis externa)- directed to the angle of mouth and give a. labialis superior et inferior, a. angularis. Veins with the same name form anastomosis between themselves and with plexus venous pterygoideus.
At the centre of regio buccalis lies corpus adiposum buccae. Between corpus adiposum buccae et buccinators lies a. et v. bucalis (a. maxillaries) et n. buccalis (n. mandibularis) - innervate tunica mucosa.
Along the line, connecting the lobe of ear with angle of mouth, passes ductus parotideus, which opens into vestibulum oris at the level of 1-2 molars.
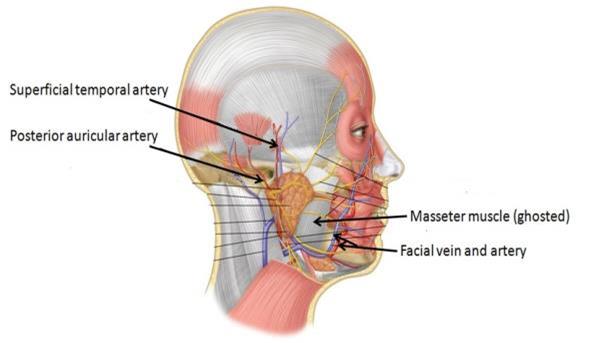
Fig 53. Region buccalis.
Тема 11.
ОБЛАСТЬ ГЛАЗНИЦЫ ( REGIO ORBITALIS).
В глазнице выделяют два отдела: поверхностный – regio palpebralis и глубокий – regio orbitalis propria, в котором находится глазное яблоко с его мышцами, сосуды, нервы и жировая клетчатка (corpus adiposum orbitae).
Regio orbitalis propria имеет 4 стенки:
1) paries superior образована os. frontalis et os sphenoidale alae minor, здесь расположена fossa gl. lacrimalis;
2) paries inferior образована facies orbitalis maxillae, здесь расположен sulcus et canalis infraorbitalis;
3) paries lateralis образована os. zygomaticus et os sphenoidale alae major, здесь расположено for. zygomaticoorbitale;
4) paries medialis образована lam. orbitalis ossis ethmoidalis et os lacrimale, здесь расположены foramen ethmoidale anterius et posterius et canalis nasolacrimalis.
На границе paries superior et paries lateralis расположена fissura orbitalis superior, через которое проходят сосуды и нервы:
1) n. oculomotorius -иннервирует mm. rectus inferior, medialis, superior et m. levator palpebrae superior et m. obliguus inferior и участвует в образовании gangl. ciliare;
2) n. trochlearis – иннервирует m. obliguus superior;
3) n. abducens – иннервирует m. rectus lateralis;
4) n. ophthalmicus – образует:
-n. frontalis, который делится на две ветви: n. supratrochlearis – иннервирует кожу верхнего века, и n. supraorbitalis - иннервирует кожу лба;
-n. lacrimalis, который иннервирует gl.lacrimalis;
-n. nasociliaris, который делится: nn. ethmoidalis anterior et
posterior – иннервирует полость носа, n. infratrochlearis -
иннервирует кожу нижнего века, r. communicans cum
gangliociliari;
5) v. ophthalmica superior – впадает в sinus cavernosus;
На границы paries inferior et paries lateralis расположена fissura orbitalis inferior, которая сообщает regio orbitalis с fossea pterygopalatina et infratemporalis. Через неё проходят: a. et n. infraorbitalis, n. zygomaticus, v. infraorbitalis.
На вершине глазничной пирамиды располагается canalis opticus,
через него проходит: n. opticus - иннервирует сетчатку глаза; a. ophthalmica – от которой отходят: aa. ethmoidales anteriore et posterior, a. supraorbitalis, suprathrochlearis, а также ветви – bulbus oculi, m. ophthalmicus, gl.lacrimalis;A. ophthalmica анастомозирует с a. dorsalis nasi.
Глазное яблоко ( bulbus oculi) сосотоит из 3 оболочек:
1) наружная – tunica fibrosa bulbi – разделена на две части: склеру (sclera) и роговицу (cornea).
2) средняя – tunica vasculosa bulbi – делится на: радужку (iris), в центре которой имеется зрачок (pupilla) вместе с m. dilatator pupillae, m. sphincter pupillae, ресничное тело (corpus ciliare) – расположено вокруг хрусталика (lens) и сосудистую оболочку (choroidea).
3) внутреняя – называется сетчаткой (retina), на ней расположено пятно сетчатки (macula), находящиеся в fovea centralis, кнутри располагается сосочек зрительного нерва (papillae nervi opticus), где отсутствует зрительное восприятие – слепое пятно (macula coeca).
Впереди lens располагается camera anterior et posterior bulbi. Основная масса bulbus oculi выполнена стекловидным телом (corpus vitreum), имеющим студенистую консистенцию.
ОБЛАСТЬ НОСА ( REGIO NASALIS).
Границы: сверху – glabella, снизу – linia horizontalis septum nasi, сбоку – sulcus nasobuccalis.
К области носа относят наружный нос (nasus externa)- состоящий из костной и хрящевой основы и полость носа (cavum nasi).
Nasus externa представлен: os nasale, processus frontalis maxillae et cartilagines nasi laterals, cartilagines alares majoris et minores. Кровоснабжение – a. dorsalis nasi (a.ophthalmica), a. angularis (a. facialis). Венозный отток по одноименным венам. Иннервация крыльев и кончика носа – n. ethmoidalis anterior, спинка носа – n. infraorbitalis.
Cavum nasi имеет 6 стенок:
1) передняя - образована nasus externa et nares;
2) задняя – образована choanae;
3) верхняя – представлена lamina cribrosa ossis etmoidalis et corpus ossis sphenoidalis, здесь расположена apertura sinus sphenoidalis;
4) нижняя – представлена palatinum durum et palatinum molle, здесь расположен canalis incisivus, for. palatinum majus et minor;
5) наружная – представлена 3 conchae nasalis superior, media et inferior, здесь расположены foramen sphenopalatinum, forr. etmoidalia anteriorus et posteriorus;
6) внутренняя – представлена septum nasi.
Cavum nasi выделяют 3 носовых хода:
- meatus nasi superior, здесь открываются cellulae etmoidales posteriors;
- meatus nasi medius, здесь открываются apertura sinus frontalis, hiatus maxillaries et cellulae ethmoidales anteriores et mediae;
- meatus nasi inferior, здесь открыватеся canalis nasolacrimalis.
Кровоснабжение стенок полости носа осуществляется ветвями a. carotis externa (a. facialis, a. maxillaries – a. spheopalatina, palatina descendens) et a. ophthalmica ( a. ethmoidales anterior et posterior, a dorsalis nasi).
Венозный отток осуществляется по одноименным венам в: plexus venosus pterygoideus et sinus cavernosus et v. facialis.
Иннервация осуществляется следующими нервами: nn. olfactorius, nn. ethmoidales anterior et posterior; rr. nasalis posteriors et n. nasopalatinum – ganglion pterigopalatinum.
ОБЛАСТЬ РТА ( REGIO ORALIS).
Regio oralis включает:
1) rima oris - содержащие в себе: - cutis, fascia superficialis, m. orbicularis oris, mm. zygomaticus major et minor, m. levator labi superioris alaeque nasi, m. levator anguli oris, m. depressor anguli oris et inferioris, здесь проходят - a. et n. labiales superior et inferior, tunica mucosa образует frenicum labi superior et inferior. Все мимические мышцы иннервируются n. facialis.
2) cavitas oris включает в себя: vestibulum oris et cavitas oris propria.
Vestibulum oris – щелевидное пространство, ограничено: снаружи – buccae, labium superior et inferior, rima oris; изнутри – dentes, gingivae, processus alveolaris maxillae, pars alveolaris mandibulae. Имеются два свода vestibulum oris superior et inferior, здесь располагаются frenulum labi superioris et inferioris. На слизистой оболочки щеки на уровне 1 или 2 верхнего моляра расположен papilla parotidea, где открывается ductus parotideus.
Cavitas oris propria – ограничено: спереди и сбоку - dentes, gingivae; сверху – palatum; снизу – fundus cavitas oris, lingua; сзади – fauces, соединяющийся с pars oralis pharynges.
Palatum durum состоит из: processus palatinus maxillae et lamina horizontalis ossis palatini образующих rafhe palati, где расположен canalis incisivus. На уровне 8 верхнего моляря расположны forr. palatina majus et minora.
Palatum molle представлена m. tensor veli palatini, m. levator veli palatini, m. uvulae, m. palatoglossus, m. palatopharyngeus. Кровоснабжение осуществляется – a. palatina descendens (a. maxillaries) – aa. palatina major et minores, a. palatina ascendens et tonsilaris (a. facialis). Венозный отток происходит в plexus pterygoideus et pharyngeus. Иннервация осуществляется ветвями ganglion pterygopalatinum – n. palatinus major et n. nasopalatinus, rr. pharyngei – n. glossopharyngei, n. vagi. m. tensor veli palatini иннервируется ветвью n. mandibularis, остальные мышцы – plexus pharyngeus.
Fundus cavitas oris образована diaphragma oris – m. mylohyoideus, здесь расположены – m. geniohyoideus et genioglossus, m. hyoglossus, m. styloglossus, m. palatoglosus – образующие основу lingua. Собственные мышцы lingua представлены – m. longitudinalis linguae superior et inferior, m. transverses linguae, m. verticalis linguae. У основания уздечки lingua открываются ductus submadibularis вместе с ductus sublingualis. Lingua кровоснабжается - a. v. lingualis, иннервация - n. lingualis (n. mandibularis), chorda tympani, n. glossopharyngeus, hypoglossus, n. laryngeus superior (n.vagus).
ЩЕЧНАЯ ОБЛАСТЬ (REGIO BUCCALIS).
Границы regio buccalis: верхняя – margo inferior os zygomaticus; нижняя - margo inferior os mandibulae; передняя – sulcus nasolabialis; задняя – m. masseter.
Кожа тонкая, эластичная, имеет волосы. В подкожной клетчатке располагаются: m. zygomaticus major, m. risorius, m. depressor anguli oris, m. buccinator, иннервирующиеся n. facialis. Под мимическими мышцами располагается межмышечное клетчаточное пространство, в котором проходят a. facialis (a. carotis externa) – направляется к углу рта и отдаёт a. labials superior et inferior, a. angularis. Одноименные вены имеют анастомозы между собой и с plexus venosus pterygoideus.
В центре regio buccalis расположено corpus adiposum buccae. Между
corpus adiposum buccae et buccinator располагается a. et v. bucalis (a. maxillaries) et n. buccalis (n. mandibularis) – иннервирующий tunica mucosa.
По линии, соединяющей мочку уха с углом рта проходит ductus parotideus, открывающийся в vestibulum oris на уровне верхнего 1-2 моляра.
LECTURE 1 2
REGIO PAROTIDEO-MASSETERICA
Regio parotideomasseterica is bounded as: superiorly - arcus zygomaticus; inferiorly - margo inferior mandibulae, anteriorly - m. masseter; posteriorly - processus mastoideus et m. sternocleidomastoideus.
Skin is thin, elastic, covered with hairs in male. Fascia parotideomasseterica covers m. masseter et glandula parotis. M. masseter is supplied with blood by a. masseterica (a. maxillaris) - passes through incisura mandibulae with v. et n. massetericus (n. mandibularis).
Glandula parotis- lies in fossa retromandibularis which contains two parts: pars profunda- reaches up to spatium parapharyngeum; pars superficialis- located on pars superficialis m. masseter. Ductus parotideus- located horizontally and laterally from m. masseter and passes through corpus adiposum buccae and m. buccinator, opening in vestibulum oris at the level of 1-2 upper molar teeth.
Following neuro-vascular formations pass through glandula parotis:
1) a. carotis externa- is divided into a. maxillaries and a. temporalis superficialis at the neck of processus condylaris os mandibulae,
2) v. retromandibularis- is formed from plexus pterygoideus (vv. maxillaries) and v. temporalis superficialis and connected with v. facialis.
3) n. facialis- forms plexus parotideus and divides into rami temporalis, rami zygomatici, rami buccales, ramus marginalis mandibulae, ramus colli, innervating mimic muscles.
4) n. auriculotemporalis- branches out from n. mandibularis and goes in regio temporalis together with a. and v. temporalis superficialis.
5) nodi lymphatici parotidei superificales et profundi.
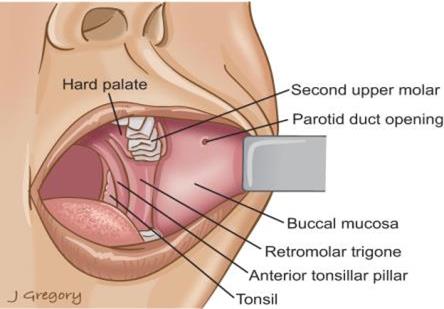
Fig 54. Regio parotideomasseterica.
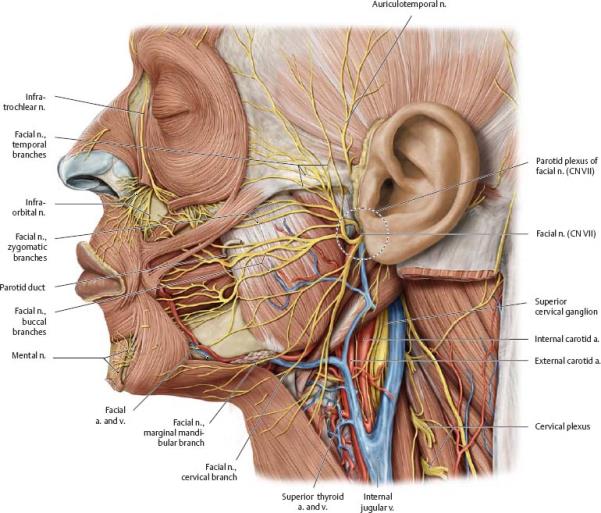
Fig 55. Regio parotideomasseterica.
DEEP AREA OF FACE (REGIO FACIALIS PROFUNDA)
Regio facialis profunda is bounded as: outside- m. temporalis, ramus mandibulae; behind- processus condylaris, glandula parotis; in front- tuber maxillae, fossa pterygopalatinum, corpus adiposus buccae; inside- lam. lateralis processus pterygoidei, m. pterygoideus lateralis, facies temporalis ala major os sphenoidale; above- basis cranii externa, fossa infratemporalis; below- place of attachment of m. pterygoideus medialis to tuberositas pterygoidea angulus mandibulae.
Regio profunda contains: a. maxillaris; plexus venosus pterygoideus, n. mandibularis, saptium temporopterygoideum, saptium interpterygoideum, spatium pterygomandibulare.
A. maxillaris branches out from a. carotis externa and goes towards for. sphenopalatinum.
There are 3 parts on its extent where arteries branch out:
a) behind processus condylaris branch out: a. alvelorais inferior, a. auricularis profunda, a. tympanica anterior;
b) between m. pterygoideus laeralis and m. temporalis branch out: a. meningea media, a. masseterica, a. temporalis profunda posterior et anterior, a. buccinatoria, a. pterygoideus lateralis et medialis;
c) inside fossa pterygopalatine branch out: a. alveolaris superior posterior, a. infraorbitalis, a. platina descendens, a. sphenopalatina.
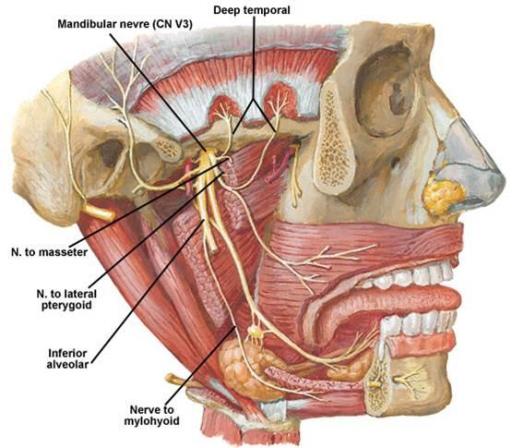
Fig 56. Mandibular nerve.
Venous blood outflow from plexus pterygoideus is carried out in v. retromandibularis and v. facialis. There are anastomoses between v. meningea media and v. opthalmica.
N. mandibularis (III ramus of n. trigeminus), is mixed, has sensitive and motor fibers. It comes out from cranial cavity through foramen ovale and in fossa infratemporalis: n. buccalis, n. auriculotemporalis, n. lingualis, n. alveolaris inferior branch out.
The tongue is innervated by n. lingualis. Chorda tympani, ganglion submandibulare (participates in vegetative innervations of tongue) are included in n. lingualis.
N. alvelorais inferior innervates mandibula. It forms plexus dentalis inferior in canalis mandibule and goes out through foramen mentale (n. mentalis), innervating skin of chin and lower lip.
N. buccalis innervates tunica mucosa buccae and cutis anguli oris.
N. auriculotemporalis innervates: articulatio temporomandibularis, porus acusticus externus, cutis region temporalis.
N. massetericus, nn. temporalis profundi, n. pterygoides lateralis et medialis innervate masticatory muscles. M. mylohyoideus, m. digastricus venter anterior are innervated by n. mylohyoideus.
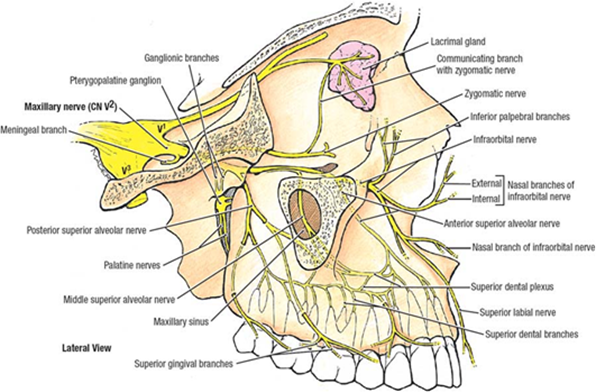
Fig 57. Trigeminal nerve.
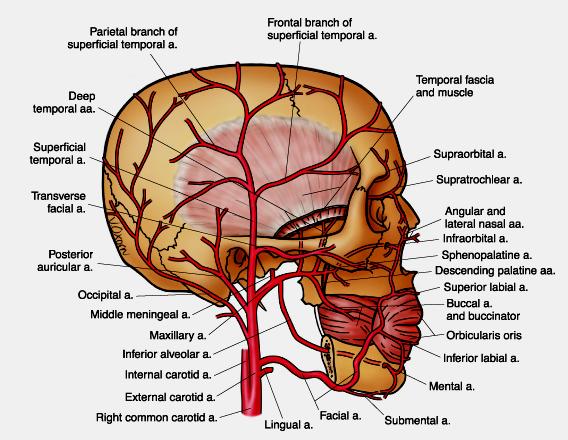
Fig 58. Faces arterial system.
PARAPHARYNGEAL SPACE
(SPATIUM PARAPHARINGEUM)
Spatium parapharyngeum is bounded as: outside- pars pharyngeum gl. paratideomasseterica, mm. pterygoideus lateralis and medialis, inside- pars pharyngeus, mm. tensor et levator veli palatine; in front- m. pterygoideus medialis; behind- fascia prevertebralis; above- fossa pterygopalatine, fossa infratemporalis; below- regio submandibularis et sublingualis.
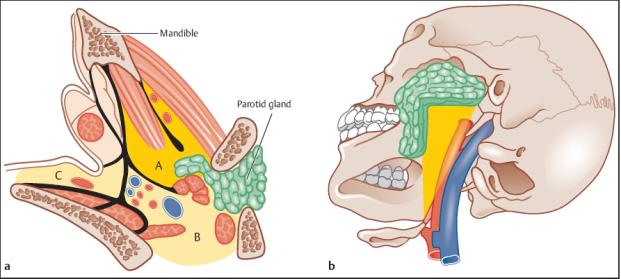
Fig 59. Parapharingeal space.
Spatium parapharyngeum consists of two sections: pars anterior and posterior, separated from each other by aponeurosis stylopharyngea.
Pars anterior spatium parapharyngeum contains: pars pharyngeum gl. parotis, a. palatine ascendens.
Pars posterior spatium parapharyngeum contains: v. jugularis interna, a. carotis interna, nn. glossopharyngeus, vagus, accessories, hypoglossus, sympathicus et nodi lymphatici profundi.
Spatium retropharyngeal is located between fascia pharyngea and fascia prevertebrale, and bounded by aponeurosis pharyngoprevertebralis sideways. It is divided by septum along median line into two sections: right and left, and hence retropharngeal abscesses are unilateral.
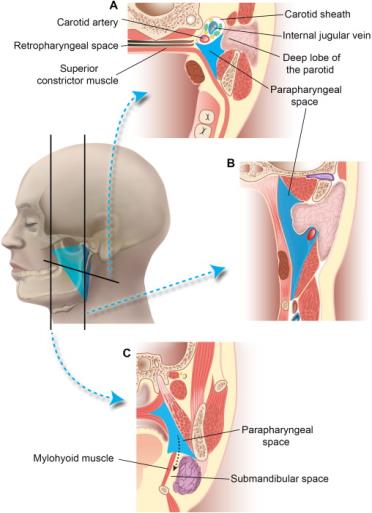
Fig 60. Parapharingeal space.
ТЕМА 12.
ОКОЛОУШНО – ЖЕВАТЕЛЬНАЯ ОБЛАСТЬ ( REGIO PAROTIDEO- MASSETERICA).
Regio parotideomasseterica ограничена: верхняя – arcus zygomaticus; нижняя – margo inferior mandibulae; передняя – m. masseter; задняя – processus mastoideus et m. sternocleidomastoideus.
Cutis тонкая, эластичная, у мужчин имеет волосяной покров. Fascia parotideomasseterica покрывает m. masseter et glandula parotis. M. masseter кровоснабжается a. masseterica (a. maxillaris) – проходит через incisura mandibulae с v. et n. massetericus ( n. mandibularis).
Glandula parotis – располагается в fossa retromandibularis, имеет две части: pars profunda – доходит до spatium parapharyngeum, pars superficialis – находится на pars superficialis m. masseter. Ductus parotideus – горизонтально и кнаружи от m. masseter, проходит через corpus adiposum buccae et m. buccinator и открывается в vestibulum oris на уровне 1 – 2 верхнего моляра.
Через glandula parotis проходят:
1) a. carotis externa - у шейки processus condylaris os mandibulae делится на a. maxillaris et a. temporalis superficialis.
2) v. retromandibularis – формируется из plexus pterygoideus (vv. maxillaries) et v. temporalis superficialis и соединяется с v.facialis.
3) n. facialis – образует plexus parotydeus и делится на rami temporalis, rami zygomatici, rami buccales, ramus marginalis mandibulae, ramus colli - иннервирующие мимические мышцы.
4) n. auriculotemporalis – отходит от n. mandibularis и направляется в regio temporalis вместе a.et v. temporalis superficialis.
5) noli lymphatici parotidei superficiales et profundi.
ГЛУБОКАЯ ОБЛАСТЬ ЛИЦА (REGIO FACIALIS PROFUNDA).
Regio profunda оганичена: снаружи – m. temporalis, ramus mandibulae;
сзади – processus condylaris, glandula parotis; спереди – tuber maxillae, fossa pterygopalatinum, corpus adiposus buccae; изнутри – lam. lateralis processus pterygoidei, m. pterygoideus lateralis, facies temporalis ala major os sphenoidale; сверху – basis cranii externa, fossa infratemporalis; снизу – место прикрепления m. pterygoideus medialis к tuberositas pterygoidea angulus mandibulae.
Regio profunda содержит: a. maxillaris; plexus venosus pterygoideus, n. mandibularis, spatium temporopterygoideum, spatium interpterygoideum, spatium pterygomandibulare.
A. maxillaris отходит от a.carotis externa и направляется к for. sphenopalatinum. На её протяжении выделяют 3 участка, где отходят артерии:
1) за processus condylaris – отходят: a. alveolaris inferior, a. auricularis profunda, a. tympanica anterior.
2) между m. pterygoideus lateralis et m. temporalis – отходят: a. meningea media, a. masseterica, a. temporalis profunda posterior et anterior, a. buccinatoria, a. pterygoideus lateralis et medialis.
3) в fossa pterygopalatina – отходят: a. alveolaris superior posterior,
a. infraorbitalis, a. palatina descendens, a. sphenopalatina.
Plexus pterygoideus – отток венозной крови осуществляется в v. retromandibularis et v. facialis, имеются анастомозы между: v. meningea media, v. ophthalmica.
N . mandibularis – (Ш – ramus n. trigeminus), смешанный, имеет чувствительные и двигательные волокна. Выходит из полости черепа через for. ovale и в fosse infratemporalis разделяется: n. buccalis, n. auriculotemporalis, n. lingualis, n. alveolaris inferior.
N. lingualis иннервирует язык. В составе n. lingualis проходят chorda tympani, ganglion submandibulare (участвующие в вегетативной иннервации языка).
N. alveolaris inferior иннервирует нижнюю челюсть. В canalis mandibulae он образует plexus dentalis inferior, выходит через foramen mentale (n. mentalis) и иннервирует кожу подбородка и нижней губы.
N. buccalis - иннервирует tunica muccosa bucce et cutis anguli oris.
N. auriculotemporalis – иннервирует articulatio temporomandibularis, porus acusticus externus , cutis regio temporalis.
N. massetericus, nn. temporales profundi, n. pterygoideus lat. et med. – иннервируют жевательные мышцы. N. mylohyoideus иннервирует m. mylohyoideus, m. digastricus venter anterior.
LECTURE 13
MASTOIDOTOMY (ANTROTOMIA)
Indicators: acute purulent inflammation of cells of processus mastoideus (mastoiditis), chronic inflammation of middle ear.
Techniques of operation:
1- arched incision of skin and subject tissues together with periosteum, on 1 cm behind the line of attachment of auricle.
2- Periosteum is removed aside by raspatory and external surface of processus mastoideus is uncovered. Within Shipo triangle, cortical layer is removed with the help of gouge and hammer. Trepanation aperture is continuously dilated to open widely the main cell of the processus mastoideus and the adjoining cells to it, containing pus- forming one big cavity. While working with cell, one should remember the location of facial nerve, sigmoid venous sinus and middle cranial fossa, which may get injured by instruments or debris. Drainage is inserted in the lower angle of the wound and 2-3 silk sutures are placed on skin.
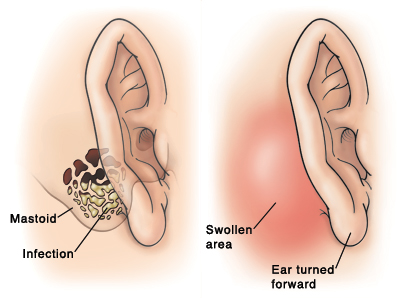
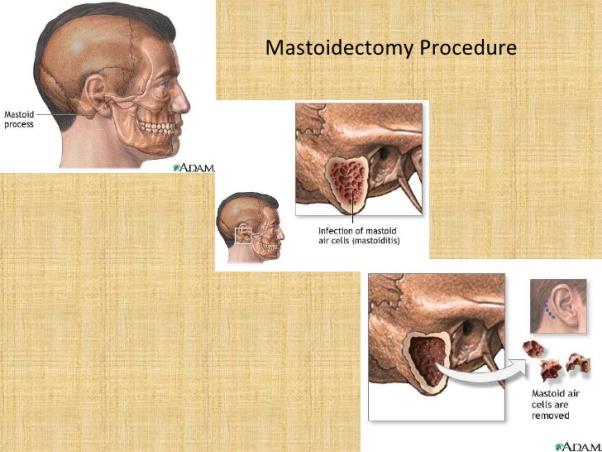
Fig 64. Mastoidectomy.
ТЕМА 13.
ОПЕРАЦИИ НА ГОЛОВЕ
ПЕРВИЧНАЯ ХИРУРГИЧЕСКАЯ ОБРАБОТКА РАН ЧЕРЕПА.
Все раны черепа подразделяются на: непроникающие (dura mater не повреждена) и проникающие (повреждена dura mater).
Первичная хирургическая обработка ран черепа – это комплекс мероприятий направленных на заживление раны. Выполняется в первые 24 часа после ранения, в отдельных случаях может производится на 2 – 3 сутки.
Техника операции при непроникающем черепно-мозговом ранении включает:
1 – бритьё волос и обработка кожи;
2 – иссечение краев поврежденной кожи шириной 0,3 – 0,5 см. окаймляющим разрезом с учетом расположения и направления хода магистральных сосудов и нервов;
3 – остановка кровотечения из сосудов подкожной клетчатки – легированием или коагуляцией;
4 – удаление из раны инородных тел, сгустков крови, нежизнеспособных тканей;
5 – края раны расширяют, удаляют свободные осколки костей и кусачками расширяют костный дефект до появления неповрежденной dura mater. Кровотечение из поврежденных v. emissaria останавливают втиранием восковой пасты или гемостатической губки, тампонированием кусочками мышцы, фасции;
6 – если dura mater не повреждена и хорошо пульсирует, её не вскрывают;
7 – ушивание раны – накладывают кетгутовые швы на galea aponeurotica и шелковые – на кожу.
Техника операции при проникающем черепно-мозговом ранении включает:
1 – все этапы операции с 1 – 5 пункты, включительно до появления dura mater, выполняются также;
6 – обработку раны dura mater начинают с осторожного удаления внедрившихся костных осколков, не меняя плоскости расположения;
7 – экономное иссечение dura mater; мозговое вещество не иссекают, а только удаляют мозговой детрит
8 – гемостаз выполняют полосками марли с раствором перекиси водорода, гемостатической губкой, коагуляцией или перевязкой сосудов;
9 – ушивают рану: редкие швы на dura mater, galea aponeurotica и кожу, в рану вставляют на 1- 2 дня резиновые полоски – выпускники.
РЕЗЕКЦИОННАЯ ТРЕПАНАЦИЯ ЧЕРЕПА (ДЕКОМПРЕССИВНАЯ).
( CRANIOECTOMIA).
Показания: повышение внутричерепного давления при опухолях, травмах, нарастающий отёк и набухание головного мозга.
Техника операции включает:
1 – бритьё волос и обработка кожи;
2 –дугообразный разрез кожи и подкожной клетчатки в правой височной области проводят соответственно прикрепления височной мышцы. Лоскут препарируют и отворачивают основанием к скуловой дуги;
3 – в вертикальном направлении рассекают височный апоневроз, межапоневротическую жировую клетчатку и височную мышцу до надкостницы. Надкостницу разрезают и распатором отслаивают на площади 6х6 или 7х7 см.
4 – ручным коловоротом просверливают в височной кости одно фрезевое отверстие, которое затем расширяют костными кусачками Борхардта, в диаметре до 6-8 см. При этом необходимо щадить a. meningea media, которая часто находится в костном канале и может быть повреждена. В случае повреждения a. meningea media кровотечение останавливают втиранием воска в костный канал. Переферический отрезок артерии лигируют или коагулируют. При повреждении артерии вне костного канала кровотечение останавливают прошиванием обоих концов артерии.
5 – после спинномозговой пункции, снижающей внутричерепное давление, рассекают крестообразным разрезом dura mater.
6 – послойно ушивают рану: кетгутовые швы на надкостницу, височную мышцу и апоневроз; шелковые – на кожу.
КОСТНО-ПЛАСТИЧЕСКАЯ ТРЕПАНАЦИЯ ЧЕРЕПА. ( CRANIOECTOMIA).
Показания: опухоли головного мозга, мозговые грыжи, водянка мозга, киста мозга и др.
Положение больного зависит от локализации патологического процесса и выбора оперативного доступа, проекция которого определяется на покровах черепа при помощи схемы Кренлейна – Брюсовой.
Техника операции включает:
1 – кожный разрез дугообразной формы проводят до надкостницы. Кожно-апоневратический лоскут отделяют и отворачивают вниз. Останавливают кровотечение. Лоскут закрывают салфеткой и прикрепляют его к операционному белью.
2 – надкостницу рассекают дугообразным разрезом, отступя от краёв раны на 1- 2 см. и распатором отслаивают её в сторону от разреза, для создания костно-надкостничного лоскута.
3 – вдоль линии разреза надкостницы просверливают 4- 5 фрезевых отверстий и кость между ними пропиливают проволочной пилой, проведенной при помощи проводника.
4 – костно-надкостничный лоскут надламывают между 1 и 5 отверстиями и откидывают книзу, сохраняя при этом его связь с надкостницей.
5 – дугообразным разрезом рассекают dura mater и лоскут отворачивают в сторону сагиттального синуса.
6 – проводят необходимые вмешательство в полости черепа. Операцию проводят осторожно, без излишней травматизации мозга, так как возможен отек мозговой ткани в послеоперационном периоде.
7 – зашивают dura mater узловыми или непрерывными швами;
8 – послойное ушивание раны.
ТРЕПАНАЦИЯ СОСЦЕВИДНОГО ОТРОСТКА.( ANTROTOMIA).
Показания: острое гнойное воспаление ячеек сосцевидного отростка (мастоидит), хроническое воспаление среднего уха.
Техника операции: делают дугообразный разрез кожи и подлежащих тканей вместе с надкостницей, на 1 см. кзади от линии прикрепления ушной раковины. Надкостницу распатором отслаивают в стороны и обнажают наружную поверхность сосцевидного отростка. В пределах треугольника Шипо с помощью долота и молотка удаляют кортикальный слой. Трепанационное отверстие постепенно расширяют, стремясь широко вскрыть основную ячейку отростка и прилежащие к ней ячейки, содержащие гной, - образуя одну большую полость. При работе с ячейками, следует помнить о расположении лицевого нерва, сигмовидной венозной пазухи и средней черепной ямки, которые можно ранить инструментами или осколками. В нижний угол раны вводят дренаж и накладывают на кожу 2-3 шва шелком.
РАЗРЕЗЫ ПРИ НАГНОИТЕЛЬНЫХ ПРОЦЕССАХ НА ЛИЦЕ.
Гнойные процессы развиваются и распространяются в подкожной, межфасциальных, межмышечных клетчатках, по ходу футляров сосудисто-нервных пучков, по фасциальным футлярам и межфасциальным щелям, через межмышечные промежутки.
Распространение гнойных процессов из первичного очага в соседние области может происходить первичным и вторичными путями. Первичными путями называют такие, по которым распространение гноя происходит без разрушения анатомических структур и элементов, по мере расплавления клетчатки в межфасциальных и межмышечных промежутках, иногда под действием силы тяжести.
Вторичными путями распространения гноя называются такие, которые сопровождаются разрушением анатомических элементов и структур (прорыв гноя из одних замкнутых фасциальных футляров в соседние), через слабые места.
Под абсцессом понимают ограниченный гнойный очаг.
Чаще всего одонтогенные абсцессы локализуются в челюстно-язычном желобке, клыковой ямке, поднижнечелюстной, щечной и околоушно-жевательной областях, реже в других участках околочелюстных тканей.
Флегмоной называется разлитое гнойное воспаление клетчатки (подкожной, межмышечной, межфасциальной и др.).
В челюстно-лицевой области нагноительные процессы разделяются на три основные группы:
1) абсцессы и флегмоны одонтогенного происхождения - остеофлегмоны;
2) абсцессы и флегмоны лимфогенного происхождения - аденофлегмоны;
3) абсцессы и флегмоны гематогенного происхождения - гемафлегмоны.
С точки зрения топографо-анатомической локализации одонтогенных
абсцессов и флегмон можно условно разделить их на две группы.
1. Околочелюстные абсцессы и флегмоны: а) тканей, прилегающих к верхней челюсти, б) тканей, прилегающих к нижней челюсти. Каждая из этих подгрупп делится на:
а) - поверхностные (а — подглазничная, щечная; б — подчелюстная, подподбородочная, околоушно-жевательная области);
б) - глубокие (а—височно-крыловидное; б - подвисочная, крылонебная ямки; в — межкрыловидное, крыловидно-челюстное и окологлоточное пространства, подъязычная область, дно полости рта).
2. Абсцессы и флегмоны соседних с околочелюстными тканями областей, куда гнойный процесс распространяется по протяжению (скуловая, височная области, глазница, позадинижнечелюстная область, шея). Абсцессы и флегмоны языка.
Абсцессы и флегмоны анатомических областей, имеют послойную структуру, топическая диагностика заключается в уточнении слоя, вмещающего очаг гнойного воспаления: подкожная, подфасциальная, межфасциальная, подмышечная или поднадкостничная клетчатка.
Основными принципами оперативного лечения гнойных процессов является широкое вскрытие гнойного очага и его дренирование, преследуя следующие цели:
а) устранение гнойно-некротического очага;
б) ограничение гнойного процесса;
в) предотвращение осложнений;
г) борьба с интоксикацией.
Разрез следует производить с учетом топографо-анатомического положения гнойного очага с сохранением целостности сосудисто-нервных пучков. При вскрытии гнойного очага должны быть соблюдены следующие требования:
1) путь к гнойному очагу должен быть коротким;
2) анатомическая целостность оперативного доступа;
3) достаточная величина разреза;
4) щадящее отношение к тканям;
5) свободный и полный отток гноя;
6) послеоперационный разрез на коже лица должен быть наименее заметен;
В челюстно-лицевой области помимо этих требований необходимо учитывать ряд анатомических особенностей:
а) поверхностное расположение крупных сосудов, нервов и их ветвей;
б) сложный рельеф костей лицевого скелета;
в) наличие клетчаточных пространств и инфицированных полостей (ротовой, носовой с придаточными воздухоносными пазухами);
г) необходимость соблюдения косметических требований.
Вскрытие гнойного очага осуществляется наружным доступом (со стороны кожных покровов) либо внутриротовым. При вскрытии поверхностных гнойников кожный разрез выполняют, исходя из топографо-анатомического расположения основных ветвей лицевого нерва и выбирая наиболее нейтральные пространства между ними.
LECTURE 1
SEPERATION OF THE TISSUES AND THE TECHNIQUES OF APPLYING SUTURES ON THE TISSUES.
Дата: 2019-03-05, просмотров: 1173.